Prognostic implications of cardiac damage classification based on computed tomography in severe aortic stenosis
Selected in European Heart Journal: Cardiovascular Imaging by M. Alasnag , S. Assiri
In the PARTNER II trial, a new staging system of extra-aortic valvular cardiac damage is proposed, using 2 D transthoracic echocardiography and its prognostic value. The purpose of this study is to evaluate the prognostic value of such extra-aortic cardiac damage using MDCT in patients undergoing TAVI.
References
Authors
Kensuke Hirasawa, Philippe J van Rosendael, Federico Fortuni, Gurpreet K Singh, Jurrien H Kuneman, E Mara Vollema, Nina Ajmone Marsan, Juhani Knuuti, Jeroen J Bax, Victoria Delgado
Reference
10.1093/ehjci/jeab071
Published
April 2021
Link
Read the abstractReviewers


Our Comment
Why this study? – the rationale/objective
Aortic stenosis is predicted to increase in prevalence with the ageing of the population. Current guidelines suggest aortic valve intervention in symptomatic severe aortic stenosis and/or left ventricular (LV) dysfunction (LV ejection fraction (EF) < 50 %). Genereux et al. proposed a new staging system of extra-aortic valvular cardiac damage using 2 D transthoracic echocardiography and its prognostic value in the PARTNER II trial. This staging system included the left atrium, right ventricle, and right atrium damages in the equation. Authors reported that the extent of cardiac damage was independently associated with increased mortality after aortic valve replacement1. The purpose of this study is to evaluate the prognostic value of such extra-aortic cardiac damage using Multidetector row computed tomography (MDCT) in patients undergoing transcatheter aortic valve implantation (TAVI).
How was it executed? – the methodology
It is a single-center retrospective study that was conducted from November 2007 to August 2019. 445 patients underwent MDCT. 40 patients were excluded due to either poor quality of the images, prior cardiac devices, or valvular procedure, or died during the TAVI procedure. 405 patients were included in the final analysis. Cardiac damage was classified into five categories:
- stage 0 (no cardiac damage),
- stage 1 (left ventricular damage),
- stage 2 (left atrium and mitral valve damage),
- stage 3 (right atrial damage)
- and stage 4 (right ventricular damage).
The primary endpoint was overall mortality after TAVI, ascertained by the patient medical records, which are linked to the governmental death registry. The stages were similar to those previously described by echocardiography (Table 1).
What is the main result?
A total of 405 were enrolled, of which 52 % were men, with a mean age of 80 +/- 7 years. 76 % had hypertension and 61 % had concomitant coronary artery disease. Although the overall ejection fraction (EF) of the studied population was 54 +/- 15 % (derived by MDCT), many had NYHA class III or IV and 82 % had hypertrophy with a mean left ventricular (LV) mass index of 90 +/- 22g/m2. Right ventricular EF (RVEF) was 48 +/- 12 %. 6.7 % were in stage 0, 23.7 % stage 1, 37.5 % stage 2, 19.3 % stage 3 and 12.8 % stage 4.
The median follow-up was 3.7 years, during which time 37 % died. The mortality was higher in stages 3 and 4, with RA and RV involvement. Other co-morbidities contributing to higher mortality included NYHA functional class > III, lower estimated glomerular filtration rate (eGFR), administration of diuretics, chronic obstructive pulmonary disease (COPD), and transapical TAVI.
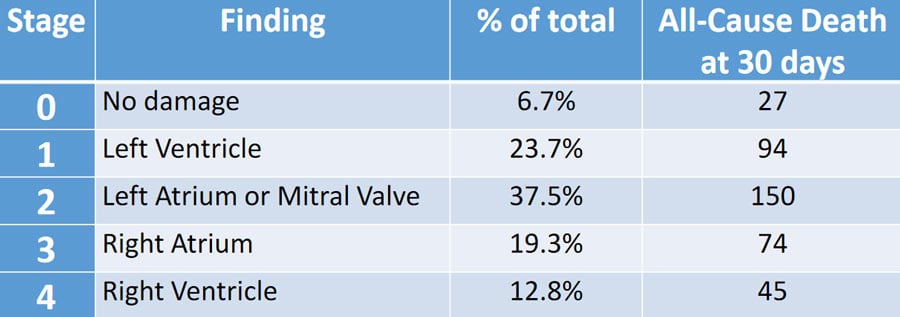
Table 1: CCT Defined Stages of Severe Aortic Stenosis
Source: European Heart Journal - Cardiovascular Imaging
Critical reading and the relevance for clinical practice:
MDCT is commonly used to evaluate patients referred for TAVI. As such, it is only intuitive to report the other parameters that may be of prognostic value for these patients, namely LV mass index, LVEF and RVEF, and volumes. This is particularly important as more studies examine early intervention, be it transcatheter (EARLY TAVR Trial) or surgical (RECOVERY Trial) replacement. Results from this study suggest that stages 3 and 4 with right-sided damage are too advanced with high all-cause mortality. The role of CCT to assess left-sided chamber volumes and function has been established in several studies with widespread adoption. However, its role for right-sided chambers, although validated, remains infrequent in clinical practice, making its adoption limited to experts invested in research or congenital heart diseases2-3. In addition, the impact of other co-morbidities, especially COPD on right-sided damage, is difficult to ascertain.
An important limitation of this study is that it was a single-center experience that does not represent contemporary practice with apical access accounting for one-third of the total population. Both a 64 and 320 slice scanners were used for image acquisition, 18 and 387 respectively. Although the number of studies performed on a 64-slice scanner was small, it is encouraging that image quality permitted obtaining the necessary measurements. The majority of patients enrolled had an eGFR that was not prohibitive for full beat acquisition protocols. Perhaps in due course more refined protocols could be adopted for high-risk individuals with iterative reconstruction and radiation reduction. Also, encouraging was the presence of atrial fibrillation in 20 % of the total population, with a higher incidence in stages 3 and 4, 50 % and 37 % respectively. Atrial fibrillation did not preclude MDCT interpretation in this study (only 7 of the total number were excluded due to poor quality images). This is certainly reassuring.
It would be valuable to understand whether these stages are dynamic, depending on the medical therapy prescribed e.g. angiotensin-converting enzyme inhibitors, regression of LV mass/hypertrophy, duration of symptoms, and time since diagnosis. Overall, the study is considered an important trial upon which more evidence can be built; a prospective multicentric trial to confirm the reproducibility of the measurements would be ideal.
References:
- Genereux P, Pibarot P, Redfors B, Mack MJ, Makkar RR, Jaber WA et al. Staging classification of aortic stenosis based on the extent of cardiac damage. Eur Heart J 2017;38:3351–8.
- Taylor AJ, Cerqueira M, Hodgson JM, et al. ACCF/SCCT/ACR/AHA/ASE/ASNC/NASCI/SCAI/SCMR 2010 appropriate use criteria for cardiac computed tomography. J Am Coll Cardiol 2010;56:1864-94.
- Gandjbakhch E, Redheuil A, Pousset F, et al. Clinical Diagnosis, Imaging, and Genetics of Arrhythmogenic Right Ventricular Cardiomyopathy/Dysplasia: JACC State-of-the-Art Review. J Am Coll Cardiol 2018;72:784-804.


No comments yet!