Severe mitral regurgitation in a patient at high risk for surgery with a suboptimal anatomy for M-TEER: what other options can we find?
This case has been accredited by EBAC with 1 CME credit
A 78-year-old male presents with recurrent hospitalisations for HFpEF and severe degenerative MR. Multimodality imaging reveals fibro-calcific leaflet disease, restricted motion, and a short posterior leaflet, making him a suboptimal candidate for M-TEER and prompting consideration of transcatheter mitral valve replacement. How would you treat?

Authors


Learning objectives
- To understand why a patient can be a suboptimal M-TEER candidate
- To explore other transcatheter options beyond M-TEER for MR treatment
- Transfemoral transeptal transcatheter mitral valve replacement can be the treatment of choice for complex MR patients
Case summary
Background
Severe mitral regurgitation
Investigation
Transthoracic and transesophageal echocardiography, cardiac CT
Diagnosis
Severe degenerative MR. Suboptimal anatomy for M-TEER due to short PML, restricted AML motion, fibrosis and calcification of the leaflets creating high risk of significant residual MR and residual stenosis
Management
Transfemoral transseptal TMVR with SAPIEN M3 system
Presentation of the case
- A 78-year-old male comorbid patient is referred for treatment after frequent recurrences of worsening hospitalisations for HFpEF:
- January 2025 – HF + COPD exacerbation → IV diuretics
- March 2025 – Anasarca, AKI on CKD, COPD flare up → IV diuretics
- May 2025 – Hospitalisation for worsening dyspnea → anasarca, severe oedema, IV continuous furosemide
- Comorbidities include dyslipidemia, obesity, COPD, permanent AF
- He has a longstanding history of CAD:
- 2006 – CABG (LIMA→LAD; sequential SVG→OM-PL)
- 03/2022 – PCI with 3 DES on SVG→OM
- 05/2022 – PCI + DES on LM–Cx
Diagnostic workup
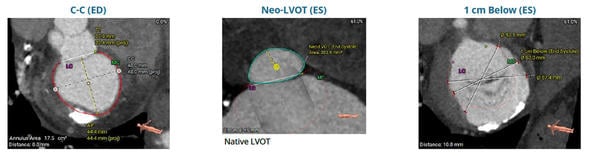
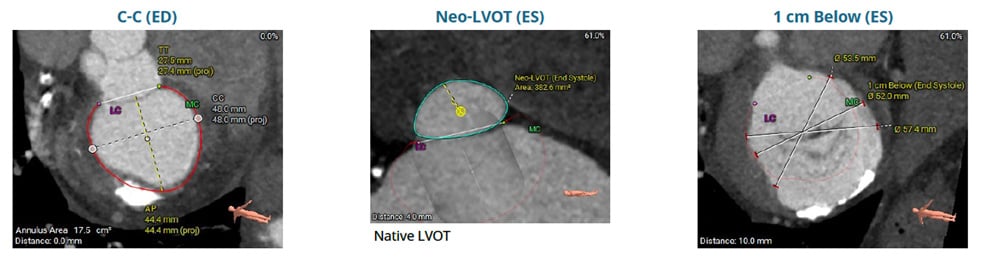
CT shows a mitral annulus with C-C 48 mm and a neo-LVOT of 382.6 mm², indicating low LVOT obstruction risk in case of TMVR. Subannular diameter at 1 cm is 52 mm
Considerations and decision
Considerations of surgical options at local heart team:
- Effective MV repair was not deemed easily feasible based on anatomy
- An effective MV repair might require long cross-clamp time and potential for repeat ECC in case of suboptimal result
- Concomitant tricuspid repair was needed in case of left heart surgery
- High surgical risk for MV replacement due to age, comorbidities, lung status and patent grafts (STS mortality 7.1%, morbidity and mortality 26.9%) with possible complications due to annular calcification
Considerations of transcatheter options at local heart team:
- M-TEER carries high risk of suboptimal results due to short PML, restricted AML motion, fibrosis and calcification of the leaflets
- High risk of significant residual MR and residual stenosis in case M-TEER was performed
- Transapical TMVR can lead to complications due to lung status and general comorbidities
- Patient had a favourable anatomy for transfemoral transseptal TMVR with the SAPIEN M3 system
Heart team consensus was to address the patient to SAPIEN M3 system implantation.
Procedural steps
Transfemoral transseptal Edwards SAPIEN M3 system implantation
Watch another case featuring the SAPIEN M3 system implantation
Declaration of interest: Dr De Marco received speaker fees and consultations for Edwards Lifesciences
Supported through a restricted educational grant from Edwards Lifesciences
To download your certificate of attendance and get your CME credits, please complete the quick satisfaction survey now!
Access here
No comments yet!