06 Apr 2022
A novel approach to left atrial appendage occlusion (when Watchman/Amulet won’t fit!)
#CardioTwitterCase originally published on Twitter
See the case of a 76-year-old female patient with mitral valve repair 10 years prior found to have incomplete surgically ligated left atrial appendage, who was referred for closure.
This case was originally published on Twitter by @dr_rothschild
Case description
Suture-based left atrial appendage surgical ligation has been demonstrated to be incomplete in up to 36 % of cases1. Closure of residual appendages remains of paramount importance to reduce future thromboembolic events, as observed in 22 % of patients with incomplete exclusion1.
We present the case of a 76-year-old female patient with mitral valve repair 10 years prior, found to have incomplete surgically ligated left atrial appendage. She was initiated on anticoagulation for a CHADS2VASC of 5, however suffered spontaneous retroperitoneal hematoma. Referred for closure.
CT with contrast was performed for pre-procedure planning (images below). Trans-septal crossing was performed with a Bayliss system.
Using fluoroscopy and 3D TEE for guidance, a 6F JR 4 placed through an 8.5F Aglis NxT was used to engage the residual appendage with a 0.035 Glide Advantage.
A 5F multipurpose catheter was advanced into the residual appendage and position was confirmed with contrast injection.
An 8F Trevisio sheath was advanced into the appendage and, in standard fashion, an 18 mm Amplatz PFO occluder was deployed with the distal disc in the appendage and the proximal disc in the left atrium.
Contrast injection confirmed placement, tug test confirmed secure hold, and the device was released.
The patient was discharged on aspirin and Plavix the following day.
Images/Videos
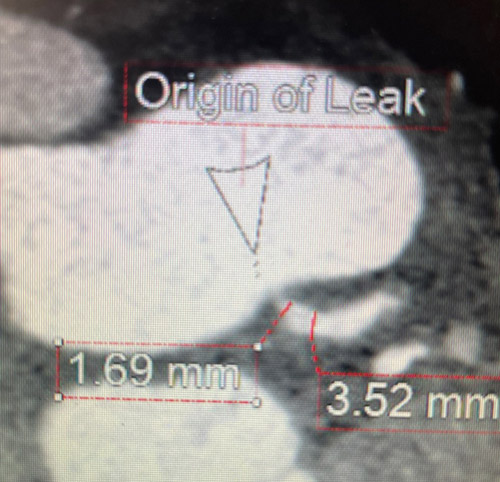
CT Angiogram Heart using Left Atrial Appendage protocol with delayed imaging for procedure planning - illustrates orfice size, origin and residual appendage depth in cross-sectional views
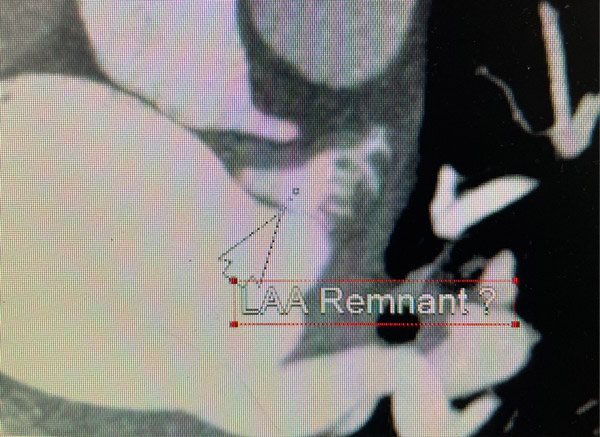
CT Angiogram Heart using Left Atrial Appendage protocol with delayed imaging for procedure planning - illustrates orfice size, origin and residual appendage depth in cross-sectional views
Final remarks
Given the reduced size of the ostium of left atrial appendage post failed surgical ligation, commercially available left atrial appendage occlusion devices were not feasible for closure.
An Amplatz PFO occluder proves to be a viable option to achieve complete occlusion of the left atrial appendage in these circumstances.
Reference
- Katz E S, Tsiamtsiouris T, Applebaum R M, Schwartzbard A, Tunick P A, Kronzon I. Surgical left atrial appendage ligation is frequently incomplete: a transesophageal echocardiograhic study. J. Am. Coll. Cardiol. 2000 Aug;36 (2):468–71.
Original tweet and Twitter discussion
Shared with patient permission - incomplete left atrial appendage surgical ligation. CT confirmed. 18mm PFO occluder placed for closure. With Dr Sean Stewart. pic.twitter.com/2eANurT9HZ
— Daniel Rothschild, MD (@dr_rothschild) March 26, 2022
Authors



1 comment
Can we use ADO II 3-4 to close it ?