15 Jun 2022
Percutaneous thrombectomy of a large thrombus in transit
Supported by the EuroIntervention Journal
View the case of a 60-year-old male patient who was diagnosed with pulmonary embolism and a large TIT, and see how he was treated by percutaneous thrombectomy.
Authors1
Maximilian Tscharre, Holger Thiele, Karl Fengler and Dmitry S. Sulimov,
Case summary
A thrombus in transit (TIT) through a patent foramen ovale (PFO) is a rare clinical finding, and rapid intervention is paramount.
Minimally-invasive percutaneous intervention modalities have evolved recently and might expand current treatment options.
We provide a case of a large TIT treated by percutaneous thrombectomy:
A 60-year-old male patient was diagnosed with pulmonary embolism and a large TIT; he was referred to our center for further therapy (Figure A).
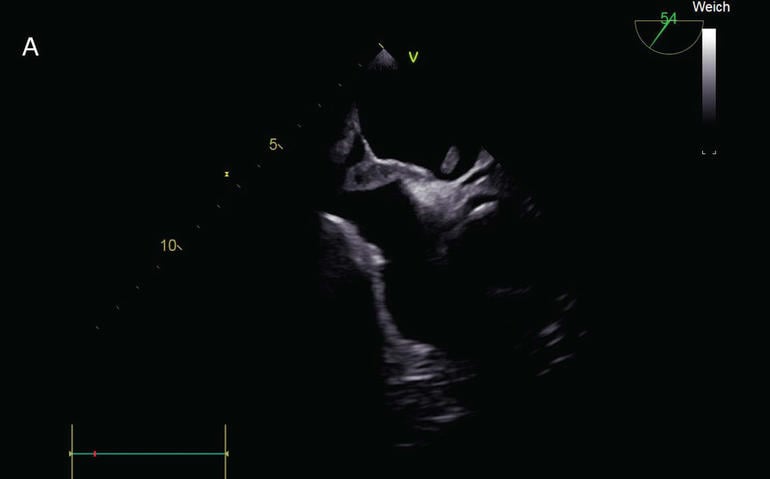
Figure A: Transesophageal echocardiography demonstrating a large thrombus in transit.
Upon arrival, the patient received 2 liters per minute of oxygen and unfractionated heparin. The Pulmonary Embolism Severity Index score equaled 90 points. Transthoracic echocardiography demonstrated right cardiac strain. Decision for percutaneous thrombectomy was made due to his high body mass index (40.1 kg/m2).
In order to prevent cerebral embolization, a TriGUARD™ protection system (Keystone Heart) was entered. Via the right femoral vein, a 20 F GORE® DrySeal Flex Introducer Sheath (Gore Medical) was inserted, and, using a 14 F Cook sheath (Cook Medical) as aspiration catheter, thrombectomy was successfully performed using the Penumbra Engine® (Penumbra Inc.), while using guidance with transesophageal echocardiography and using VacLoc® syringes (Merit Medical Systems) for the introducer sheath.
A large thrombus was retrieved (Figure B).
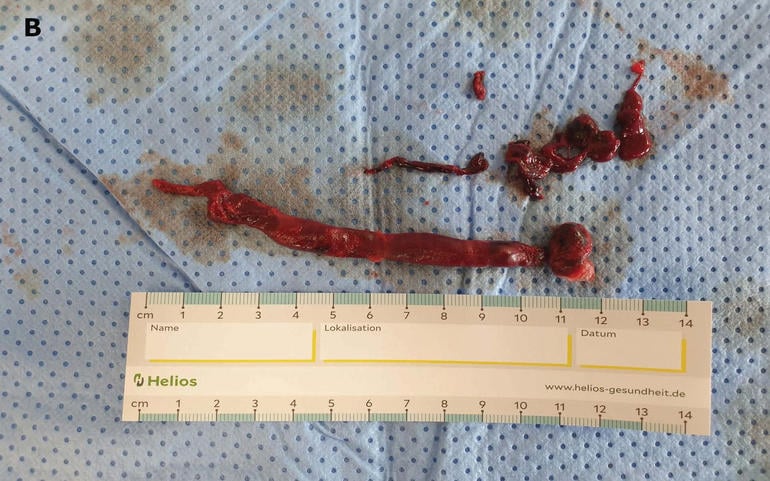
Figure B: Large thrombus retrieved by percutaneous thrombectomy.
After the intervention, the orientating neurological examination was unremarkable.
Oral anticoagulation was started and the patient was discharged four days after intervention. Elective PFO closure was advised.
Conclusion
Treatment of a TIT is time-sensitive because of the high risk of systemic embolism. Common therapy options include systemic anticoagulation, thrombolysis, or surgical thrombectomy, however, as the detection of a thrombus in transit is a rare finding, no definite consensus upon optimal treatment strategy is available1,2.
Based on small investigations, surgical thrombectomy is preferred due to increased mortality risk, and risk for embolization with thrombolysis or anticoagulation1,2.
However, the advent of percutaneous devices might offer new minimally-invasive treatment modalities for TITs.
Best to our knowledge, no data on percutaneous thrombectomy for the treatment of a TIT have yet been reported.
According to our case, percutaneous thrombectomy seems feasible and might expand current treatment options. However, more data are necessary in order to evaluate the merit of percutaneous thrombectomy in patients with thrombi in transit.
References
- Myers PO, Bounameaux H, Panos A, Lerch R, Kalangos A. Impending Paradoxical Embolism. Chest. 2010;137:164–70.
- Fauveau E, Cohen A, Bonnet N, Gacem K, Lardoux H. Surgical or medical treatment for thrombus straddling the patent foramen ovale: Impending paradoxical embolism? Report of four clinical cases and literature review. Archives of Cardiovascular Diseases. 2008;101:637–44.
Affiliations
- Department of Internal Medicine/Cardiology, Heart Center Leipzig at the University of Leipzig
Conflict of interest statement
The authors do not have conflicts of interest
1 comment
Good management