Post-dilation from contralateral access site for nose cone entrapment during self-expandable transcatheter aortic valve implantation
Supported by the EuroIntervention Journal
View this successful case with bail-out post-dilation for modifying nose cone entrapment due to stent frame infolding.
Authors1
Hirofumi Hioki, Yusuke Watanabe, Hideyuki Kawashima, Akihisa Kataoka, Ken Kozuma.
Case summary
An 84-year-old female, who had hypertension and diabetes mellitus, was admitted to our hospital undergoing transcatheter aortic valve implantation (TAVI).
Pre-procedural computed tomography demonstrated that perimeter of aortic annulus was 66.8 mm (area 336 mm2) and anatomy of lower limb was suitable for transfemoral (TF) access.
Therefore, we performed TF-TAVI using the Evolut PRO+ 26 mm (Medtronic) after pre-dilatation, using a 17 mm balloon based on the minimum diameter of annulus.
Because the valve dived deeply during deployment, we recaptured it 2 times and could finally deploy at a preferable position using cusp-overlap technique.
After the deployment, we started to remove delivery catheter system, however, nose cone of the catheter got stuck in the valve due to stent frame infolding, and we could not advance and remove it anymore (Figure 1A).
Figure 1: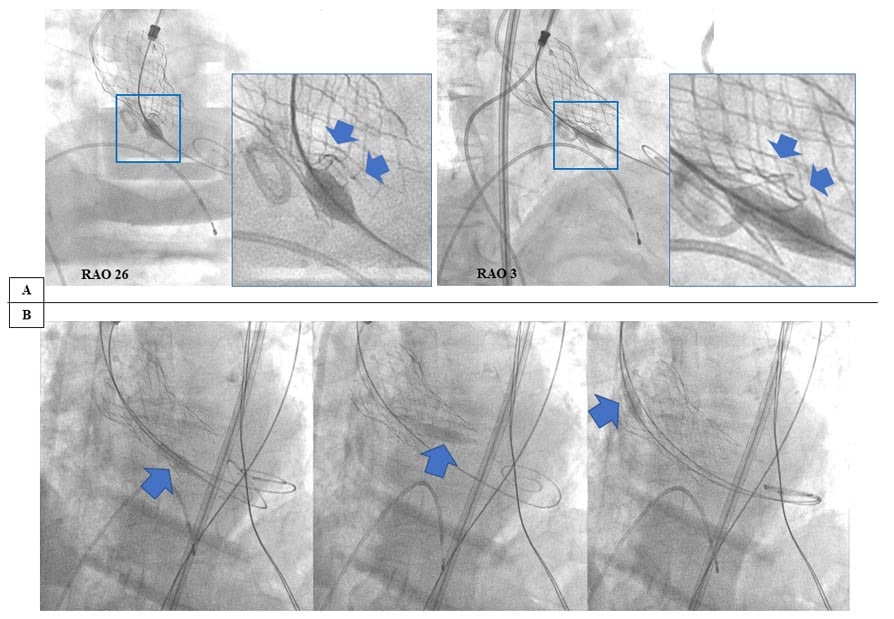
(A) Nose cone entrapment. Blue arrows indicate stent frame infolding.
(B) Nose cone retrieve. After post-dilation, infolding stent frame was fixed (left side panel) and nose cone was easily centralized, resulted in removing from heart valve (middle and right side panels).
To prevent valve embolization by pulling the system forcefully, we tried to modify the infolding by post-dilation, using an 18 mm balloon from contralateral femoral access (Moving image 1).
By attempting this procedure, the infolding frame was released and we could retrieve the nose cone of delivery catheter without additional effort (Figure 1B) (Moving image 2).
Here, we firstly described a successful case with bail-out post-dilation for modifying nose cone entrapment due to stent frame infolding of the Evolut PRO system.
Though nose cone entrapment by infolding during TAVI using Evolut PRO system has not been reported, this situation has a risk of valve embolization when the system is forcefully removed.
In this case, we speculated stent frame infolding might be caused by a relatively small pre-dilation balloon or recapture maneuver, resulting in nose cone entrapment1. To manage this, post-dilation from contralateral access site may be feasible and effective strategy to modify the infolding.
Conflict of interest statement
None of the authors has relevant conflict of interest to disclose.
References
- Ancona MB, Beneduce A, Romano V, Buzzatti N, Russo F, Bellini B, Ferri LA, Agricola E, Landoni G, Scandroglio AM, Chieffo A, Montorfano M. - Self-expandable transcatheter aortic valve infolding: Current evidence, diagnosis, and management. Catheter Cardiovasc Interv 2020. doi: 10.1002/ccd.29432.
Affiliations
- Division of Cardiology, Department of Internal Medicine, Teikyo University Hospital, Tokyo, Japan.


No comments yet!