Recurrent common femoral artery stenosis after surgical knot closure: Cut the knot using directional atherectomy
Supported by the EuroIntervention Journal
A 70-year-old man without history of peripheral arterial disease presented with severe claudication six months after TAVI which was performed via surgical cut-down common femoral artery access site…
Authors
Wai Kin Chi1, GM Tan1,2, Chak-Yu So1,2, Bryan P Yan1,2,3
Case summary
A 70-year-old man without history of peripheral arterial disease presented with severe claudication (Rutherford Class 3) six months after transcatheter aortic valve implantation (TAVI) which was performed via surgical cut-down common femoral artery (CFA) access site. Surgical access was performed under direct visualization via a skin incision and subcutaneous tissue dissection with subsequent femoral artery exposure and closure afterwards.
Pre-TAVI computerized tomography showed the right CFA was normal in calibre (7mm) without stenosis or calcium. Duplex ultrasound (DUS) showed focal stenosis over right CFA. Invasive peripheral angiogram showed severe focal right CFA stenosis (Panel A, yellow asterisk). Plain old balloon angioplasty (POBA) was performed using a 7 x 40mm non-compliant balloon (Mustang, Boston Scientific, MA, USA) with satisfactory angiographic results (Panel B).
The patient’s claudication symptom recurred nine months after POBA. Second invasive angiogram revealed severe restenosis in the right CFA (Panel C, yellow triangle). Directional excisional atherectomy (HawkOne™, Medtronic, MN, USA) was performed with distal embolic protection (SpiderFX, Medtronic, MN, USA) to treat the CFA restenosis (Panel D).
A 7x60mm drug-eluting balloon (IN.PACT Admiral, Medtronic, MN, USA) was applied afterwards. Final angiographic result was satisfactory (Panel E).
Examination of debris excised by the atherectomy device revealed fibrotic tissue and specks of blue coloured foreign material suggestive of retained surgical stitches (Panel F, yellow arrow).
Patient remained symptom-free at one year and follow-up DUS showed normal peak systolic velocity (PSV) over right CFA.
Access site vessel injury due to endovascular treatment is not uncommon and often under-diagnosed. The use of directional atherectomy followed by balloon angioplasty is considered to be a safe and effective endovascular approach to treat femoral artery occlusion related to vascular closure devices.
However, its application for vascular complication secondary to surgical knot closure has not been reported. Treating this type of complication with POBA alone may be inadequate to relieve vessel constriction by physical stitches, leading to restenosis.
Among the different atherectomy devices available on the market, probably only the directional atherectomy device offers the features needed for treatment of this specific surgical-knot-closure-associated femoral artery occlusion.
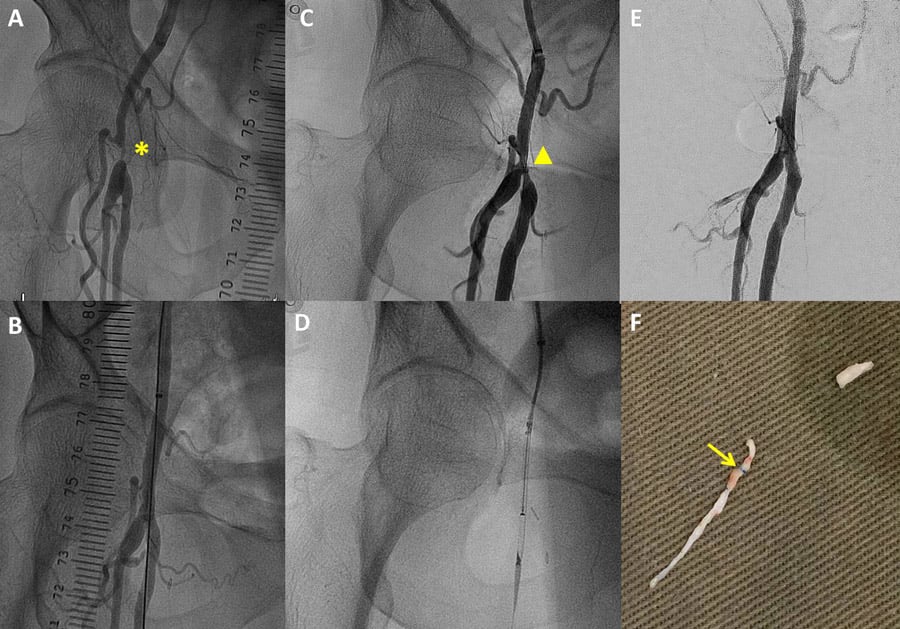
Figure 1. A) Angiogram showed severe focal right CFA stenosis (yellow asterisk). B) Satisfactory angiographic result was achieved after POBA. C) Second angiogram revealed restenosis in the right CFA (yellow triangle). D) Directional excisional atherectomy was performed. E) Final angiographic result was satisfactory. F) Examination of debris revealed suspicion of retained surgical stitches (yellow arrow).
Conflict of interest statement
The authors have no conflicts of interest to declare.
Affiliations
- Division of Cardiology, Department of Medicine and Therapeutics, Prince of Wales Hospital, Hong Kong Special Administrative Region, People’s Republic of China
- Institute of Vascular Medicine, The Chinese University of Hong Kong, Hong Kong Special Administrative Region, People’s Republic of China
- Department of Epidemiology & Preventive Medicine, School of Public Health, Monash University, Melbourne, Australia
No comments yet!