09 Sep 2024
How to deal with ilio-femoral tortuosity during TAVI procedure: the buddy wire technique to straighten the pathway
A problem-solving step by step tutorial
Frequency of the problem:
Expert level:
Summary
Aortic and ilio-femoral tortuosity are common challenges encountered during transcatheter aortic valve implantation (TAVI). Several techniques can be employed to overcome this challenge and successfully complete the procedure.
The Problem
Extreme bilateral ilio-femoral tortuosity and calcification can hinder the advancement of sheaths and prosthesis (Figure 1).
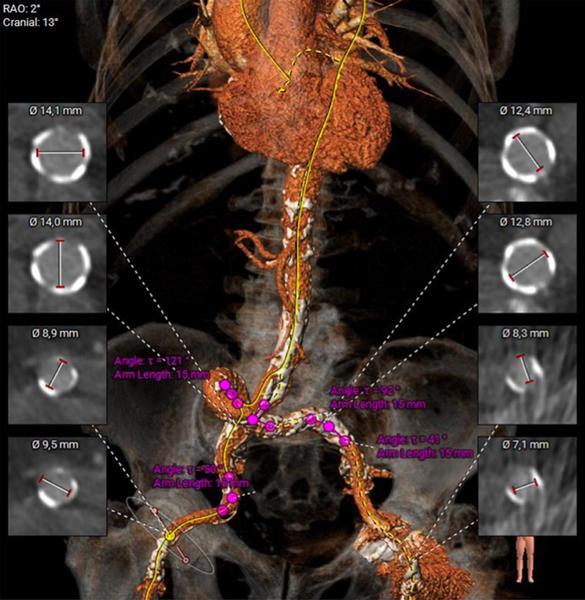
Figure 1: CT analysis of the ileo-femoral axis, revealing an extremely tortuous and calcified ileo-femoral pathway

Principal idea
The primary goal of our strategy is to straighten the ilio-femoral axis and provide maximum support to facilitate the advancement of large sheath and prosthesis.
Material needed
- A 6 Fr introducer sheath.
- A 6 Fr multipurpose guiding catheter.
- Two stiff guidewires.
Method step-by-step
Step 1
A 6 Fr introducer sheath is placed after echo-guided femoral artery punction.
A 6 Fr multipurpose guiding catheter is advanced over a regular 0.035” J guidewire and parked in the thoracic descending or the abdominal aorta.
Step 2
A stiff guidewire (e.g. Lunderquist® extra-stiff wire guide, Cook Medical) is placed within the multipurpose catheter through the aorta until it reaches the aortic root (Video 1).
Step 3
A second stiff guidewire is advanced through the multipurpose catheter into the aorta, parallel to the first guidewire. Retract the guiding catheter and the introducer that was in place from the beginning of the maneuver, ensuring both wires remain in position (Video 2).
Step 4
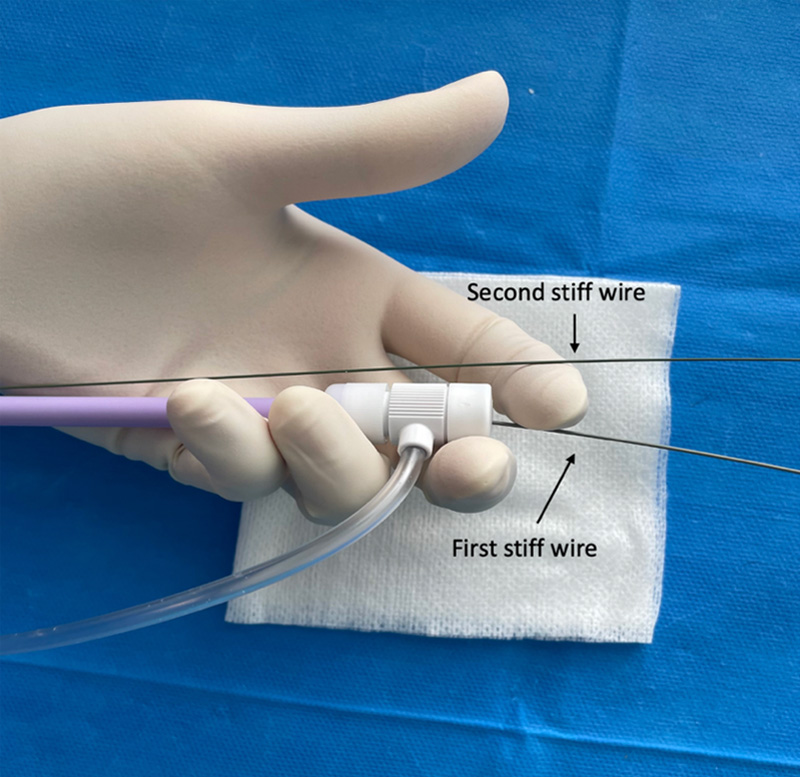
Advance the introducer sheath (in our case a 14 Fr) over one of the two stiff guidewires. The second wire remains in the arterial system, parallel to the sheath, and externalized on the operating table (see Video 3 and Figure 2).
The second wire can be gently retrieved once the introducer is in place.
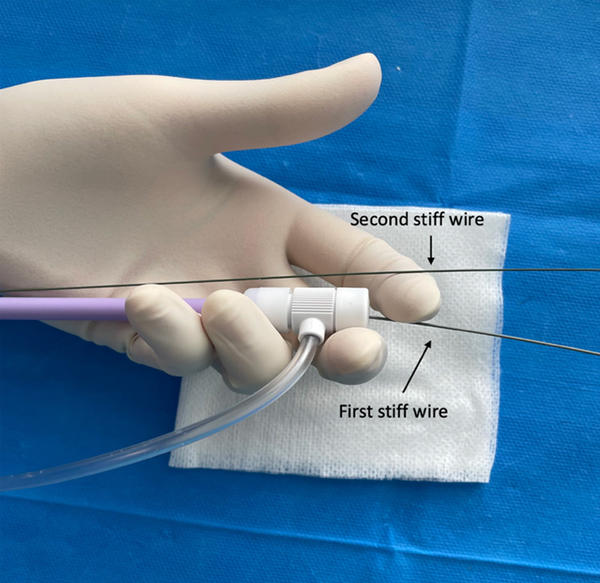
Figure 2: the first stiff wire is placed into the introducer. The second stiff wire is kept outside the introducer and left in contact with the arterial wall
Points of specific attention
- It can be employed either as an initial strategy or as a "bail out" option when the standard method is ineffective.
- Consistently monitor the advancement of the stiff wires with X-rays due to the risk of dissection and perforation, particularly when the vessel has severe calcification.
- Be mindful of the “concertina effect”, also named “accordion effect”, which describes the angiographic appearance of tortuosity in an artery when it is crossed and stretched by a wire. This phenomenon can occur when a wire straightens the artery, leading to the invagination of tissue.
A word from the reviewer - Radoslaw Parma

Double guidewire techniques are essential in the training for coronary and structural heart disease interventions. They allow to straighten vascular anatomy to facilitate device deliverability.
The presented the iliofemoral double wire technique is essential for aortic interventions and has several advantages:
- It avoids additional arterial puncture to allow second wire insertion
- The catheter use ensures no harm to the aortic wall occurs during stiff wire placement
- It reduces arterial wall contact with the TAVI delivery system across the abdominal and thoracic aorta.
The procedure may pose some minor risks:
- in narrow, heavily calcified and tortuous iliac arteries, where the femoral sheath may press the buddy wire against the surrounding calcium, potentially leading to wall dissections
- Although unlikely, the presence or movement of the buddy wire may widen the access site dimensions in extremely fragile femoral artery tissue.
- Wire placement in the aortic arch may pose additional stroke risk, which may be avoided by its positioning distal to the left carotid artery
Thank you to the Toulouse Team for sharing precious advice that is indispensable for SHD operator training.
Authors





1 comment
great tips & tricks...