19 Jan 2026
How to manage Safari wire entrapment during TAVI with Navitor THV
A problem-solving step-by-step tutorial
Safari wire entrapment during TAVI is a rare but potentially serious complication, particularly with sheathless self-expanding valves. In this My Toolkit article, we describe a simple, effective technique using a parallel stiff guidewire to safely retrieve both the catheter and the entrapped Safari wire when performing TAVI with the Navitor THV—while preserving vascular access.
Frequency of the problem:
Expert level:
Summary
Entrapment of the Safari wire within the transcatheter heart valve (THV) delivery system is a rare but potentially serious complication. It can occur when the Safari wire tip is damaged, preventing its removal from the valve delivery system.
If this happens during the use of a sheathless self-expanding THV, the operator may have no alternative but to remove both the THV catheter and the entrapped Safari wire, resulting in loss of vascular access. To address this issue, we propose a simple yet effective solution when using the Navitor platform. The integrated sheath of the Navitor system provides sufficient lumen space to introduce a 0.035” stiff parallel wire. This allows the operator to safely retrieve both the catheter and the entrapped Safari wire while maintaining a bailout wire for vascular access management.
The problem
After valve implantation, the Safari wire can be removed from the left ventricle by re-advancing the THV delivery system through the valve. When the Safari wire is retracted within the THV catheter, a complication may arise: the wire may become entrapped due to a kinking inside the THV catheter, preventing its removal.
In cases where a sheathless self-expanding THV is used, the only remaining option may be to remove the entire catheter with the Safari wire still inside, relying solely on the pre-closure, without a bailout wire for vascular access management.
Principal idea
If the Safari wire becomes entrapped within the catheter of a Navitor THV, a bailout 0.035” stiff guidewire can be introduced through the system's integrated sheath. This parallel wire advances within the space between the inner wall of the integrated sheath and the catheter shaft, entering the iliofemoral axis.
This simple yet effective maneuver may allow the operator to safely remove both the catheter and the entrapped Safari wire while preserving vascular access.
Material needed
- 0.035” stiff guidewire (e.g. Amplatz Super Stiff™, Lunderquist Extra-Stiff®, etc.)
Step-by-step method
Step 1
When the Safari wire is removed from the left ventricle by re-advancing the THV delivery system through the valve (Video 1), it may become entrapped due to a kinking within the THV catheter, preventing its removal (Figure 1).
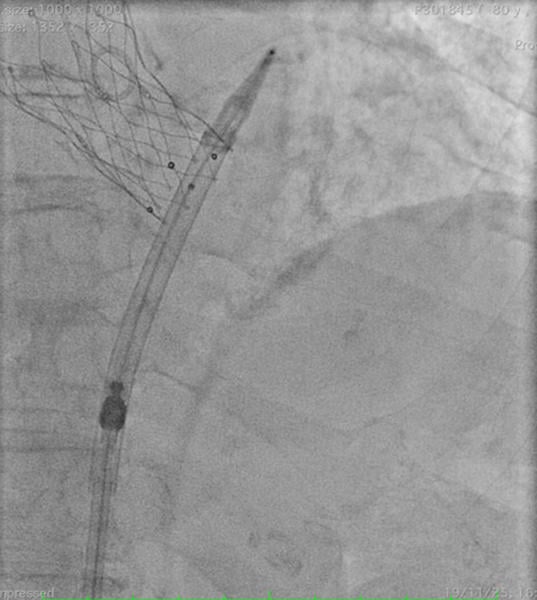
Figure 1

Step 2
A 0.035” stiff wire can be inserted in parallel, through the integrated sheath of the Navitor THV (Video 2). The wire can traverse the sheath only when the valve capsule is not fully retracted against the distal tip of the sheath (Figure 2, Video 3).

Figure 2

Step 3
Both the catheter and the Safari wire can be safely removed while maintaining a bailout wire for vascular access management (Video 4).
Points of specific attention
- The proposed technique is applicable to all Navitor valve sizes (23, 25, 27, 29 and 35 mm), as both integrated sheath sizes (14 Fr and 15 Fr equivalent) provide adequate space for the advancement of a 0.035“ parallel guidewire.
- It is important to note that the wire can traverse the sheath and reach the aorta only when the valve capsule is not fully retracted against the distal tip of the sheath.
- It is worth noting that this technique cannot be performed with the Evolut platform, as its integrated sheath lacks the necessary space to accommodate a parallel wire.
A word from the reviewer

This tutorial describes a bail-out option in the event of wire entrapment with the Navitor Flexnav delivery system that allows preservation of the main vascular access. Wire entrapment may result from a damage to the wire surface due to increased manipulation of the delivery system, particularly in complex and tortuous vasculature.
However, the maneuver described by the authors to re-advance the delivery system into the left ventricle to retrieve the Safari wire is rather questionable. It is more common to first withdraw the delivery system and then exchange the wire over a pigtail catheter.
As a matter of fact, wire entrapment is a rare complication, but once it occurs, may unnecessarily complicate the procedure and eventually have deleterious consequences. Even after the valve is deployed, maintaining vascular access is essential as the procedure must still be completed, including assessment of the valve function, management of underexpansion or malpositioning, and safe closure of the femoral access. When using plug-based closure device, loss of wire may even preclude vascular closure.
Hence, simply the knowledge that the integrated sheath provides sufficient lumen space to introduce a 0.035” stiff parallel wire may be useful to prevent more severe complications or laborious maneuvers once this problem occurs. Obviously, this technique does not require advanced skills.
The insertion of a stiff 0.035” wire via the introducer of a 4 or 5 French sheath may provide more stability and could avoid damage to the wire tip. Particular attention should be paid when the wire exits the sheath within the iliac artery.
It is important to note that the described technique works with the Navitor Flexnav system, but not with other self-expanding devices with integrated sheath as these typically lack sufficient internal lumen space to allow introduction of a 0.035“ parallel wire.
In conclusion, the authors should be congratulated for introducing this technique that complements the interventional armament for successful management of complex TAVI procedures.
Conflict of interest
Dr. Won-Keun Kim declares having received proctor/speaker honoraria from Abbott, Anteris, Boston Scientific, Cardiawave, Edwards Lifesciences, Jenavalve, HID Imaging, Medtronic, Meril Life Sciences, P & F. Institutional fees from Boston Scientific.
Disclosures
All authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Authors






2 comments
fully endorsed
Is there enough space in the Evolut platform to use a 0.014" extra-stiff wire in order to maintain access?