Porcelain aorta, calcified aortic valve, and calcified left main: what comes first, the valve or the artery?
Euro4C Case
How would you treat this 76-year-old male patient with severe AS symptomatic for angina, sinus rhythm with RBBB, previous bilateral CEA, and total occlusion of both the left CCA and the subclavian?

Authors



Valve or artery first?



Clinical presentation
- 76-year-old male patient
- Absolutely “fit”
- Severe AS symptomatic for angina (CCS class-II and worsening to class-III + NYHA class II in the last 6 months)
- LV function (EF 55 %), renal GFR (50 ml/min)
- Sinus rhythm with RBBB (with risk of total AV-block)
- Previous bilateral CEA
- Doppler: total occlusion of the left CCA, and total occlusion of the subclavian (and vertebral left artery)
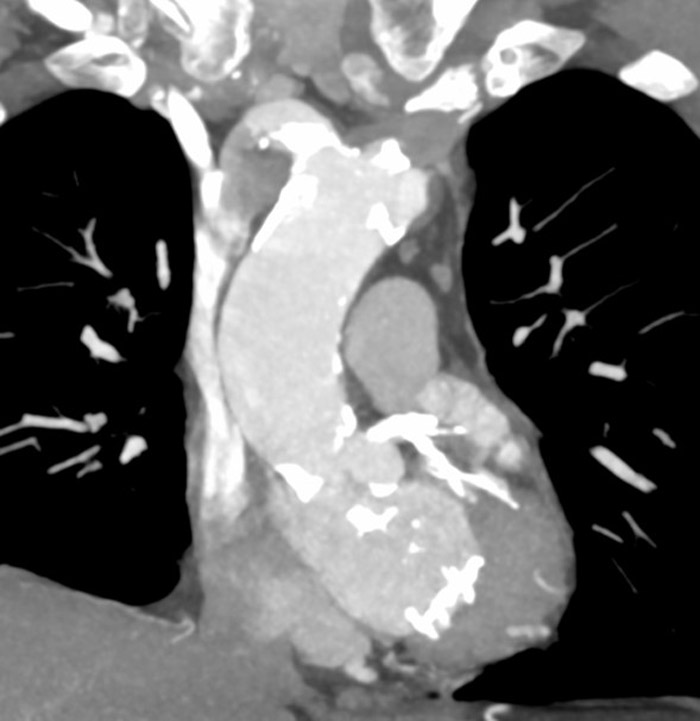
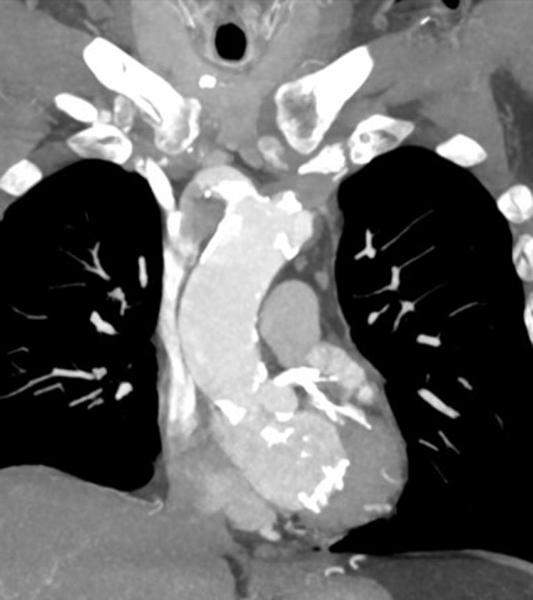
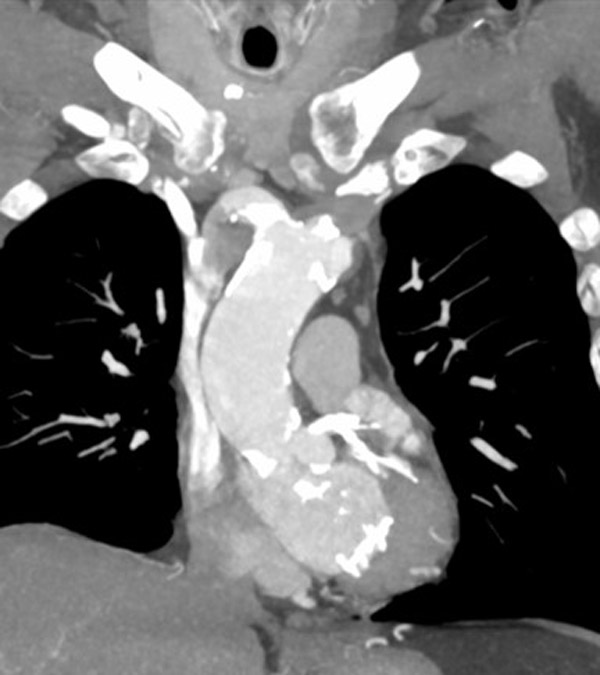
CT scan
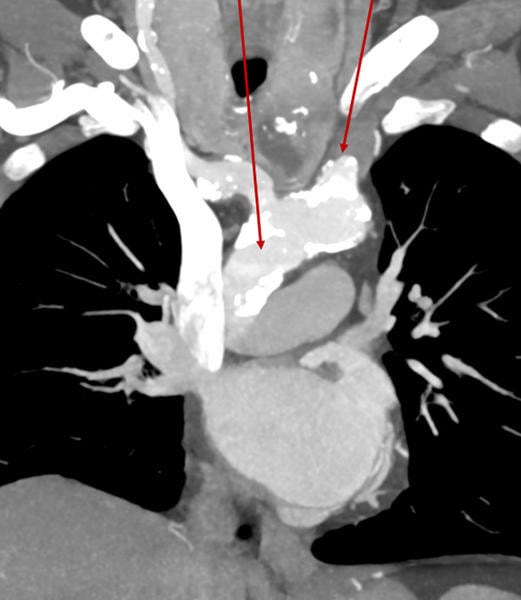
Porcelain aorta and occluded left common carotid artery
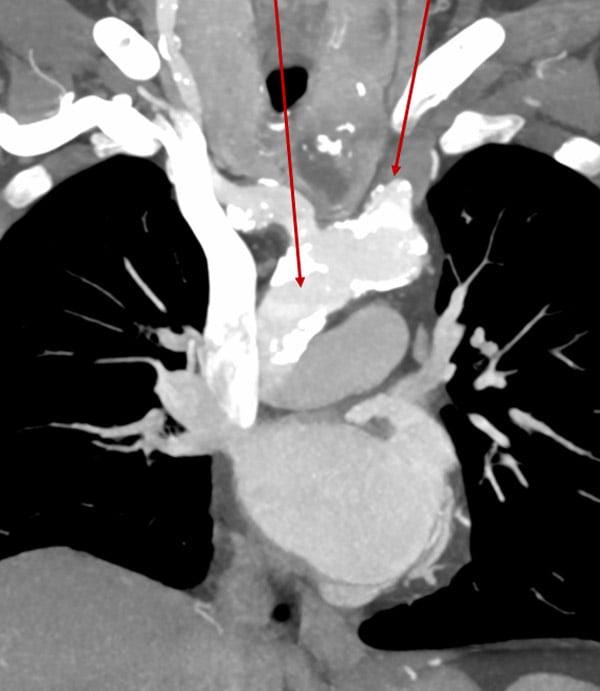

Occluded subclavian artery

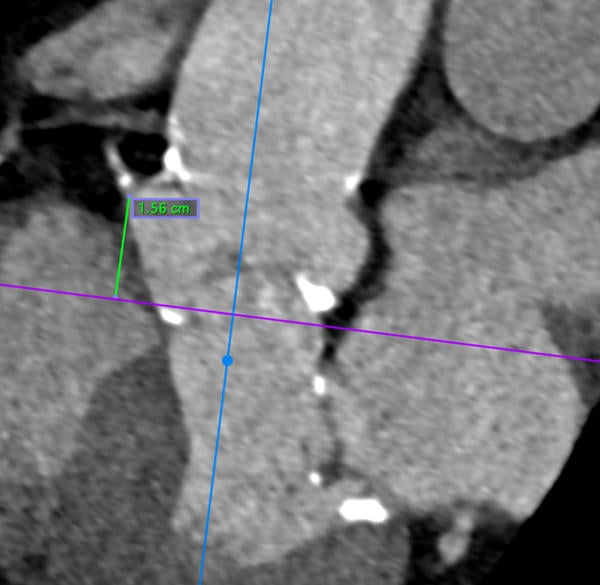
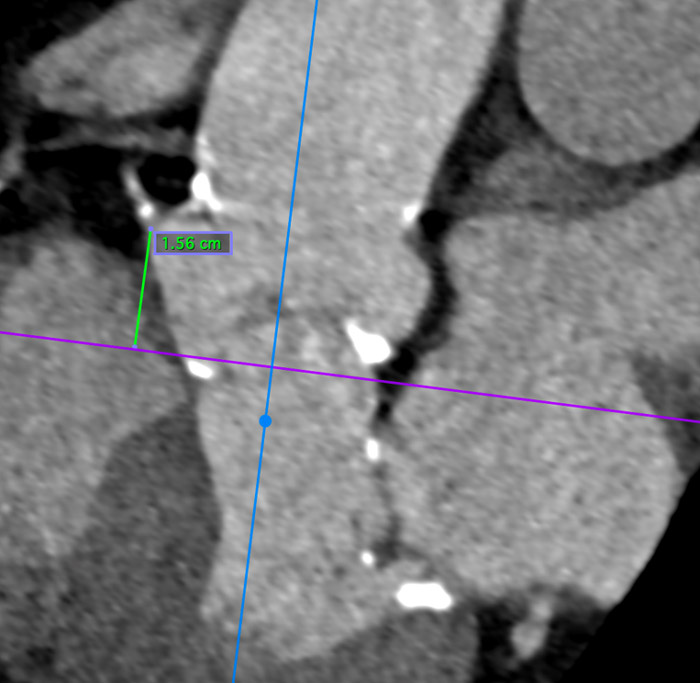
Calcified LVOT
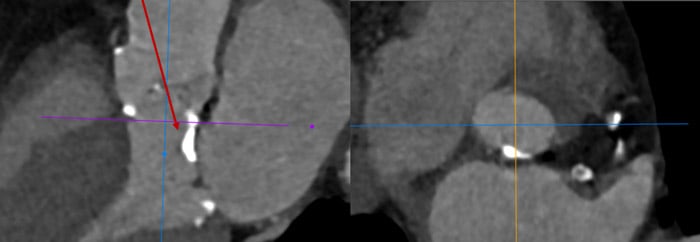
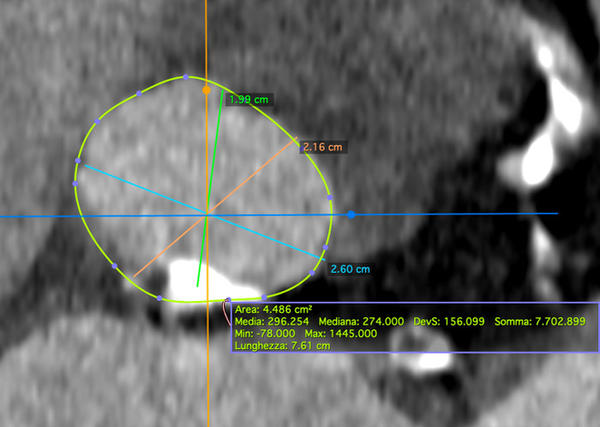
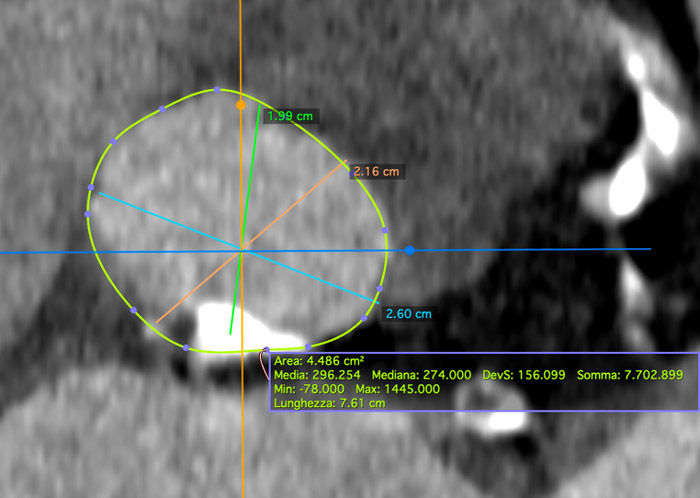
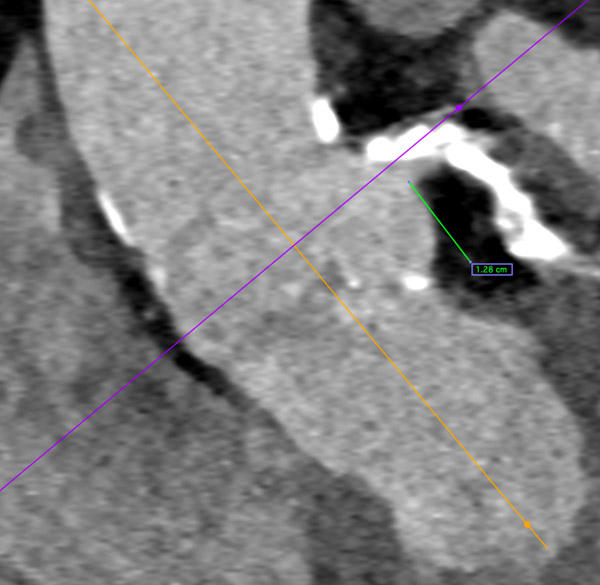
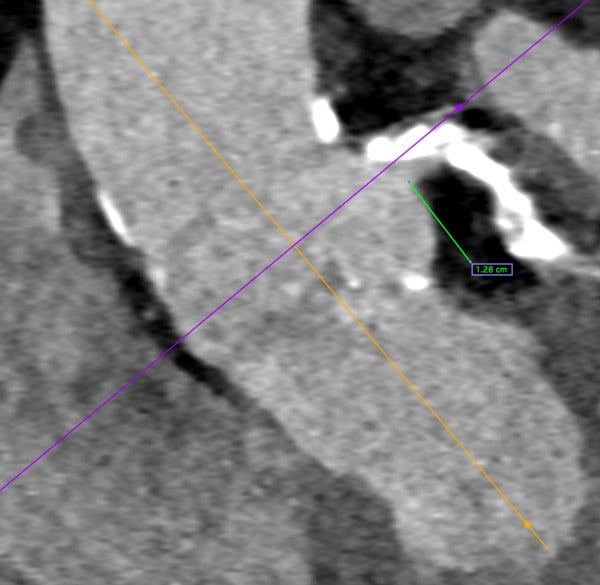
Valve sizing and LM calcification
LVOT
RCA
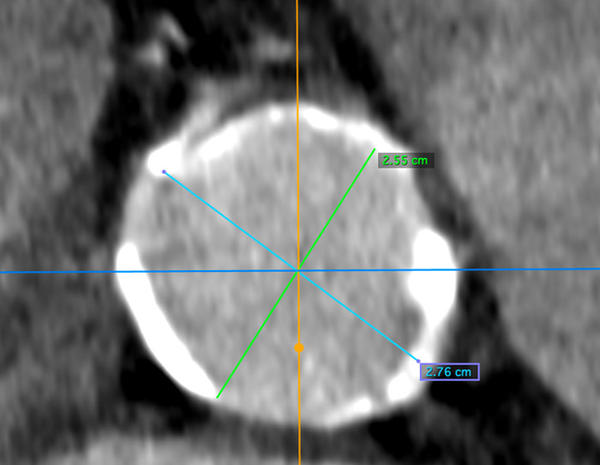
STJ
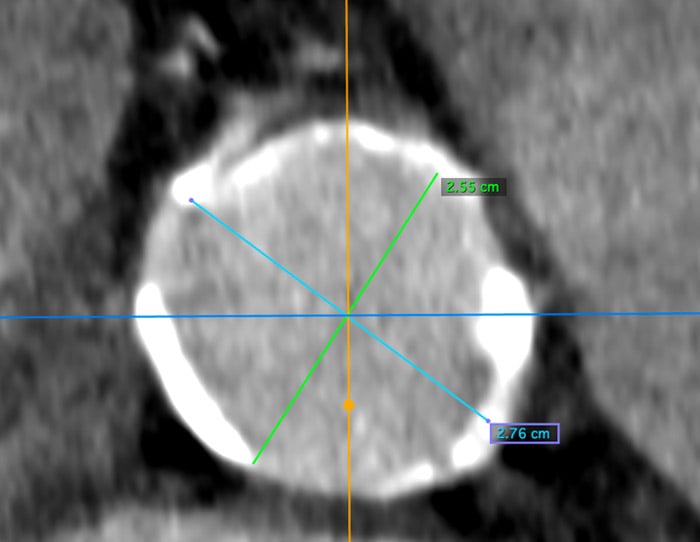
Massive calcification of the LM and LAD/LCx
LCA

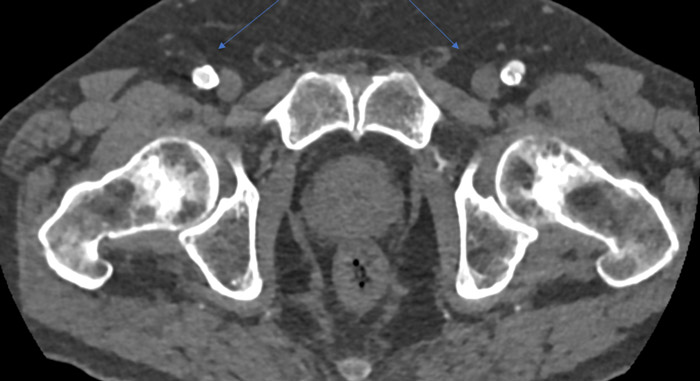
Calcified aorta and iliacs

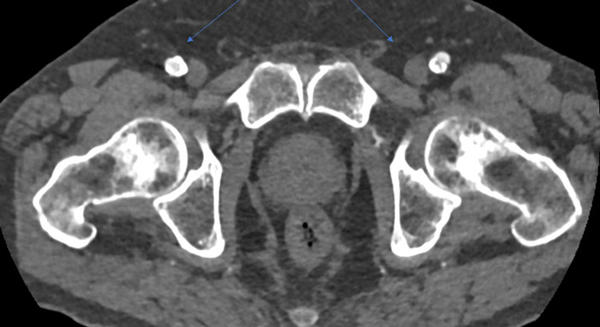
Common femoral arteries
Coronary angiogram
Severe disease of the anonymous trunk and occlusion of a minor RCA
Heart Team meeting
Despite the "youngish" aspect of the patient, and the “low” surgical risk, SAVR + CABG x 3 in a man with porcelain aorta and occlusion of 2/4 epi-aortic vessels was considered to have an unfavourable risk balance, compared to combined TAVI + PCI endovascular approach.
However, different endovascular teams would plan this case differently…
Tell us how would you manage this case!
How would you treat? (please, answer question 1 to discover the next one!)
Powered by Quiz MakerSupported through a restricted educational grant from Medtronic.
Learning objectives:
- How to treat CAD in patients with severe calcified AS: why, when, and how?
- How to facilitate access to coronaries after implantation of a THV
- How to perform a complex PCI after implantation of a THV
No comments yet!