The future of aortic valve replacement - From index procedure to lifetime management
A 68-year-old woman presents with symptomatic aortic stenosis and tricuspid valve anatomy, with no significant comorbidities and no evidence of coronary artery disease. Given her strong preference for a less invasive strategy, the Heart Team considers a transcatheter approach.
How would you treat this patient—and in case of TAVI, which prosthesis design would you choose?
Authors



- In February 2026, a 68-year-old woman was referred to our center for evaluation regarding aortic valve replacement.
- Her primary care cardiologist had been aware of her aortic valve stenosis for some time; at her last follow-up visit, there was clear clinical and echocardiographic progression of the condition.
- At the time of her presentation at our institution, she was in NYHA Class III with no signs of decompensation. Her general and nutritional status is normal for her age (height 164 cm, weight 60 kg).
- The following are relevant comorbidities:
- History of transient ischemic attack without neurological sequelae
- Osteoporosis
- Polyarthrosis (bilateral shoulder TEP, planned knee TEP) with chronic pain syndrome
- Hypertension
- Blood test results:
- Creatinine: 73 mmol/L
- GFR: 72 mL/min
- NT-proBNP: 296 pg/mL
- Hb: 10.7 g/dL
- HC: 0.30
- Platelets: 319 × 10^9/L
- White blood cells: 8 × 10^9/L
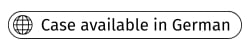
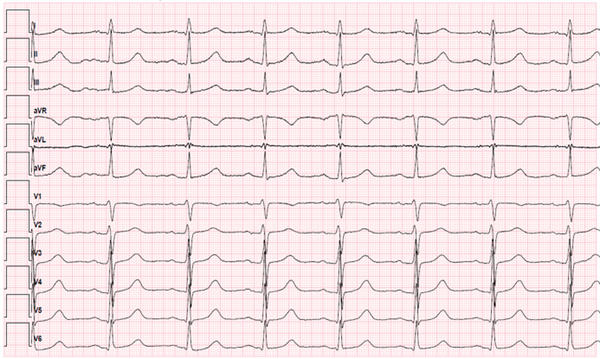
ECG
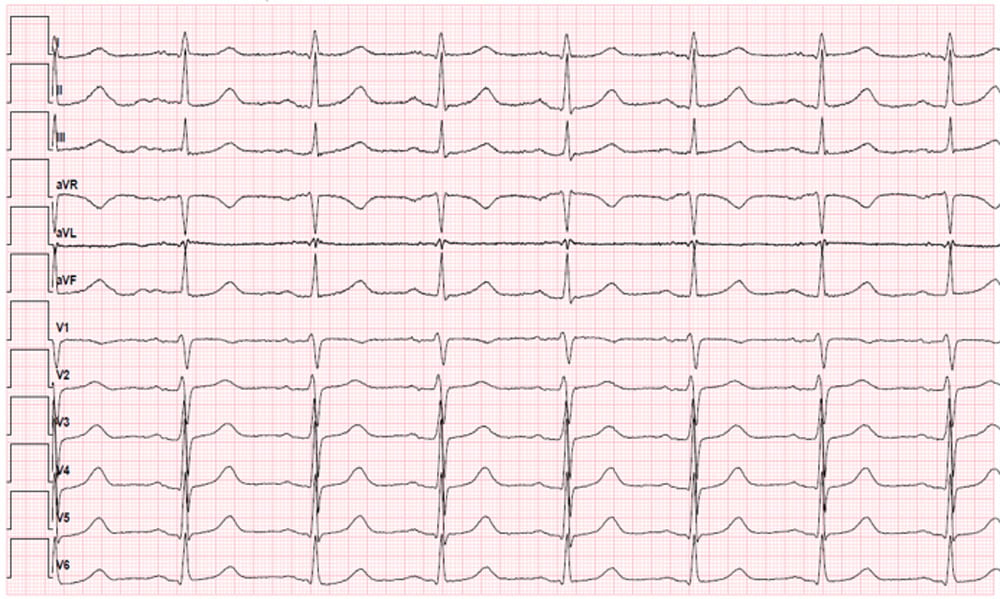
Echocardiography
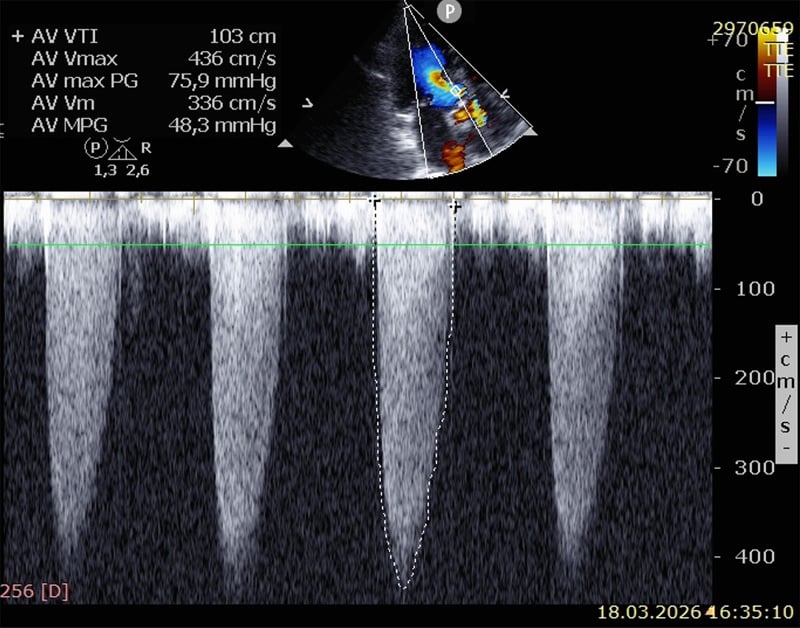
- Normal systolic left and right ventricular function (EF ~ 65%)
- Moderate concentric hypertrophy
- High-flow aortic valve stenosis (maximum gradient 76 mmHg, mean gradient 48 mmHg, no aortic valve insufficiency)
- Grade I mitral and tricuspid valve insufficiency
- Estimated pulmonary artery pressure ~ 25 mmHg
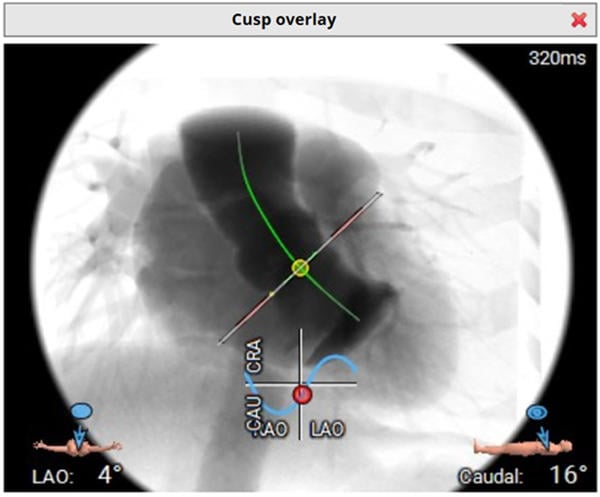
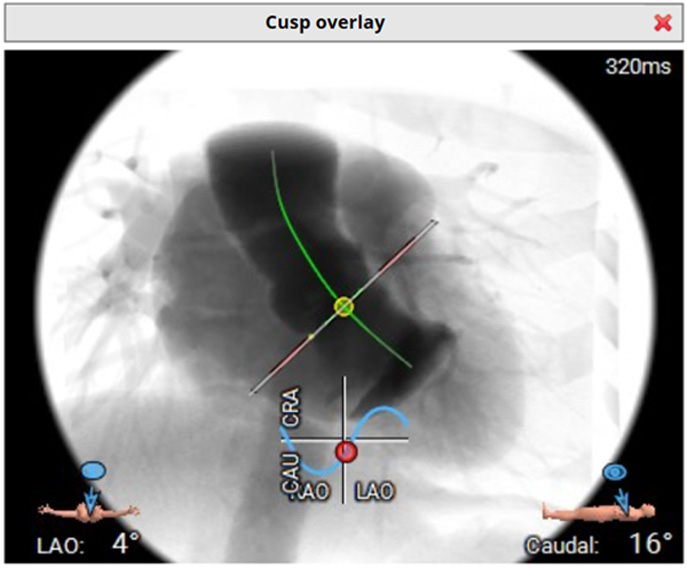
Coronary angiography
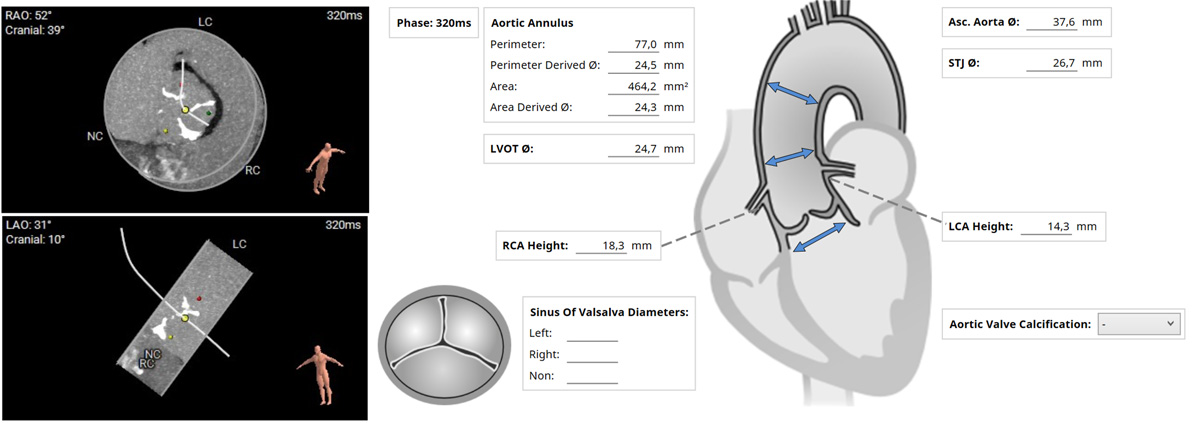
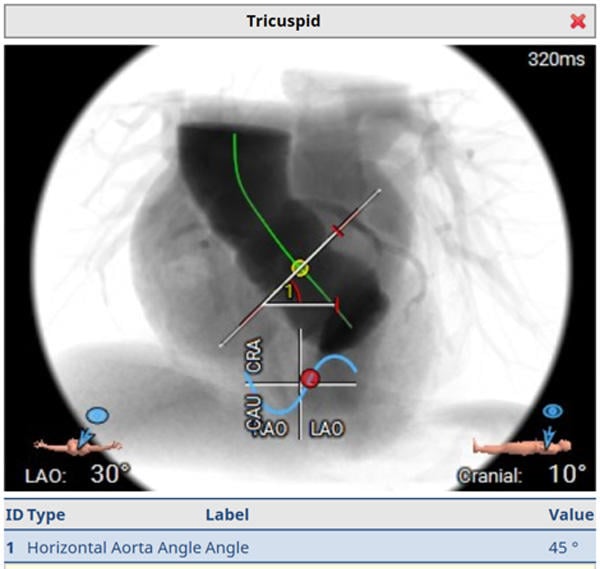
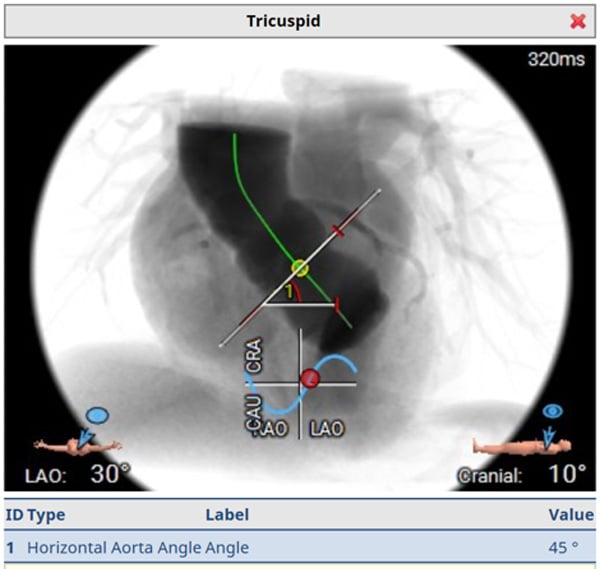
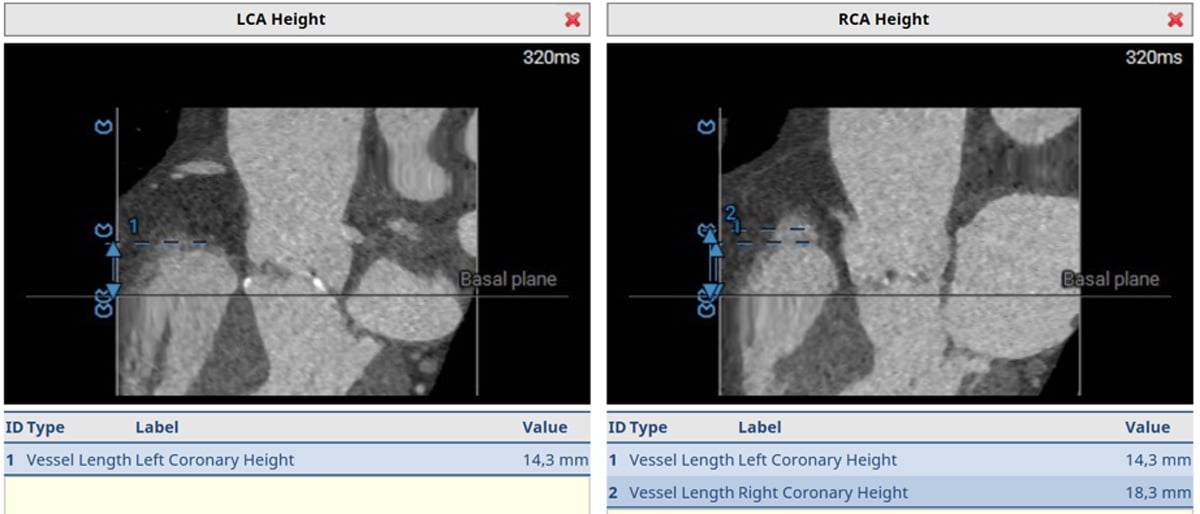
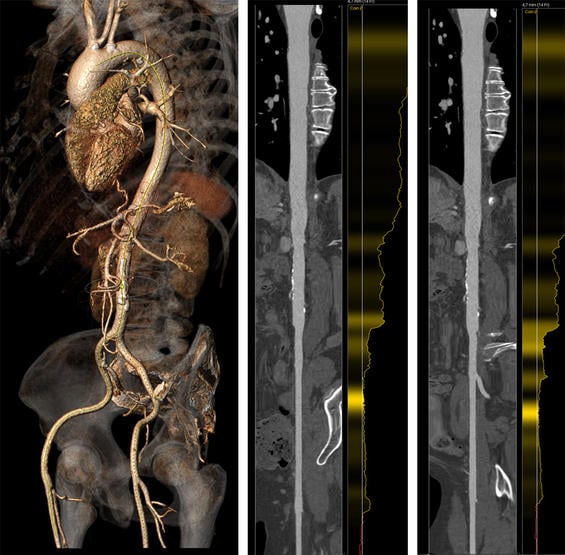
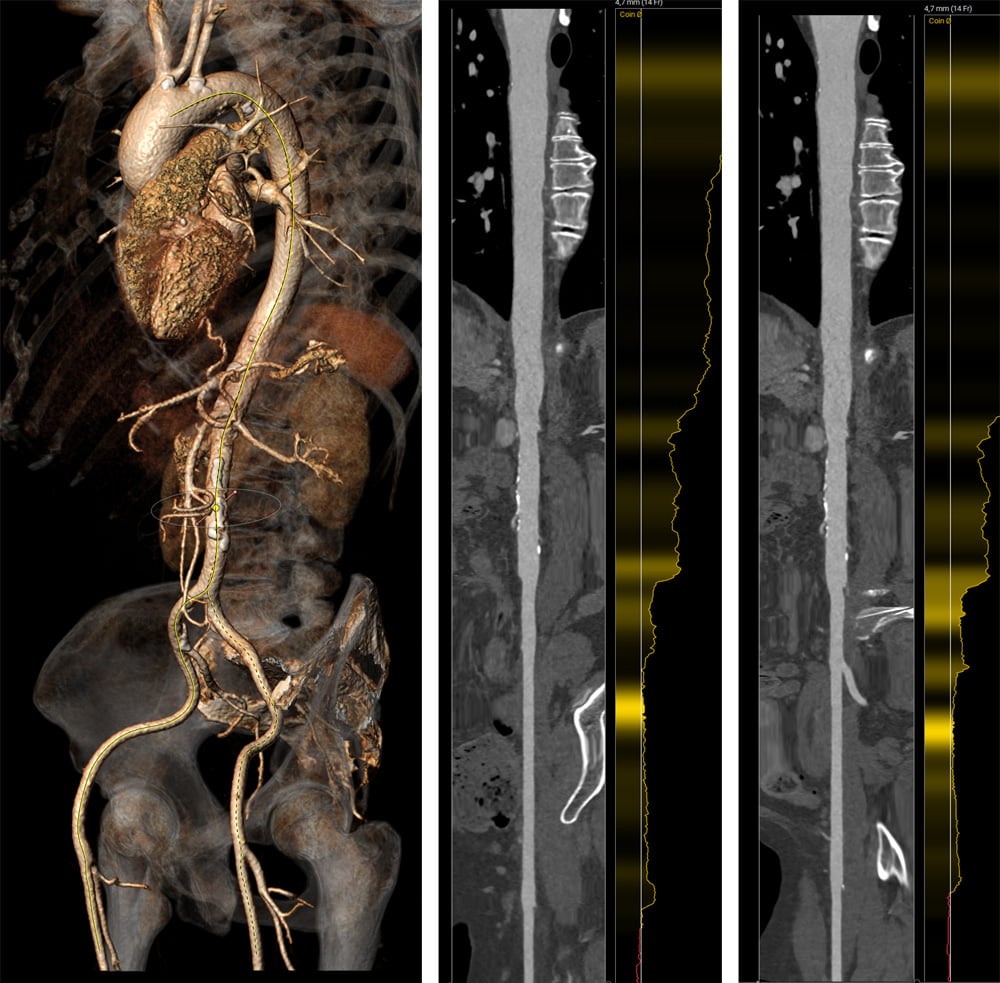
Computed tomography
- Summary + Heart Team evaluation:
- 68-year-old woman with symptomatic aortic valve stenosis and tricuspid valve anatomy
- Coronary artery disease ruled out; no relevant comorbidities
- Strong patient preference for interventional approach
Learning objectives
- Describe the role of the multidisciplinary Heart Team in the evaluation and treatment planning of intermediate and low risk patients undergoing TAVI
- Outline the key principles of lifetime management in intermediate and low-risk TAVI patients and contrast these with management strategies in high-risk populations
- Understand how artificial intelligence-based tools can support clinical decision-making in patient selection, procedural planning and long-term management of low and intermediate-risk TAVI patients.
Dr. Buckert reports the following disclosures:
- Invited talks: Shockwave Medical; Daiichi-Sankyo; AstraZeneca; Boehringer Ingelheim; Abbott; Medtronic; Bristol-Myers-Squibb, Alnylam, Bayer, Zoll, Amgen
- Travel grants: Bayer Vital; Pfizer; Boehringer Ingelheim; Abbott; Medtronic; Boston Scientific; ASAHI INTECC
- Advisory boards: Pfizer, Bristol-Myers-Squibb
No comments yet!