09 Dec 2022
First half of DK-Crush technique for bailout stenting of a true 0,0,1 bifurcation
#CardioTwitterCase originally published on Twitter
Stent implantation is largely debated in true 0,0,1 bifurcation lesion. This case shows bailout IVUS-guided stenting of a large diagonal branch after DEB-induced dissection, performed by employing the first half of the DK-Crush technique, thus avoiding stenting in the disease-free left anterior descending artery.
This case was originally published on Twitter by @giuseppe_ando
Case description
Percutaneous coronary intervention (PCI) with stent implantation in true non-left-main 0,0,1 bifurcation lesion is associated with unfavorable outcomes, and potentially higher mortality.
Therefore, a consensus exists that, if deemed indicated, PCI for 0,0,1 lesion should be limited to balloon-based techniques, ideally consisting in plaque modification with cutting/scoring balloon of the side branch (SB), and final treatment with a drug-eluting balloon (DEB).
We present the case of an 80-year-old male with troponin-positive acute coronary syndrome (Video 1) due to a culprit lesion in the ostium of a large diagonal branch (DIAG). IVUS evaluation demonstrated no significant disease (Figures 1, 2, 3) in the left anterior descending artery (LAD) and a mixed plaque in the DIAG, whose reference diameter was > 3 mm.
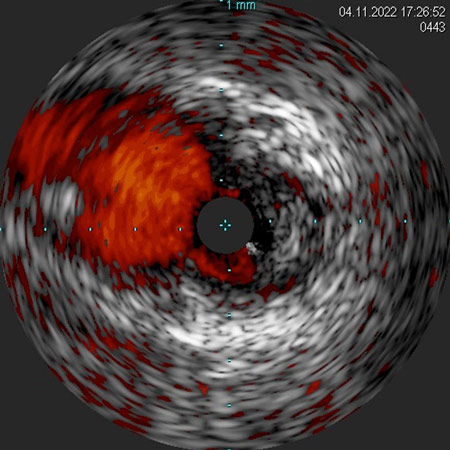
Figure 1: IVUS pullback from the DIAG with ChromaFlo imaging. A mixed plaque causing a significant stenosis of the DIAG ostium is evident. The LAD appears free of significant atherosclerotic disease.
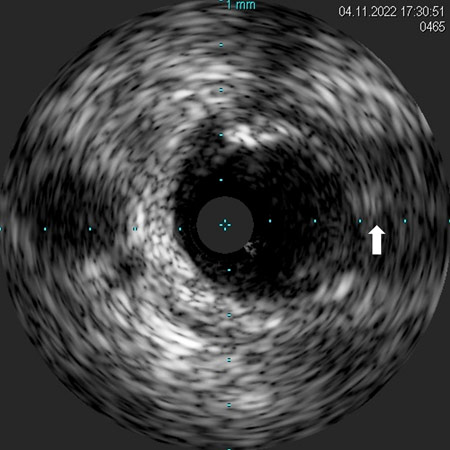
Figure 2: IVUS pullback from the LAD. The still frame corresponds to the LAD segment immediately distal to the DIAG ostium. The arrow indicates the DIAG wire.
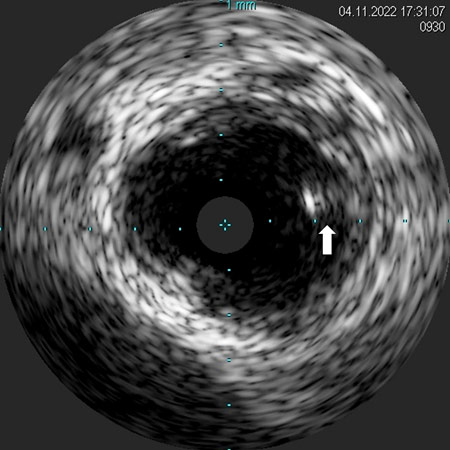
Figure 3: IVUS pullback from the LAD. The still frame corresponds to the LAD segment immediately proximal to the DIAG ostium. The arrow indicates the DIAG wire now into the LAD.
As the patient was highly symptomatic, PCI was indicated, and the plan was to sequentially dilate the ostial lesion of the DIAG with undersized balloons and finish the procedure with a 1:1 DEB inflation, thus avoiding stent implantation.
The ostial DIAG lesion was dilated with a 2.0 mm and a non-compliant 2.75 mm balloons, obtaining a modest luminal gain. Then, a 3.0 mm DEB was inflated at nominal pressure for 60 seconds. The angiographic control demonstrated a spiral dissection in the DIAG (Video 2), thus bailout stenting of the DIAG was deemed necessary.
A 3.0 x 16 mm DES was placed at the DIAG ostium with minimal protrusion into the LAD, where a balloon was parked uninflated. The DES was implanted in the DIAG and a first kissing-balloon inflation was performed. After DIAG wire removal, DES struts were crushed by the LAD balloon. Then, proximal rewiring of the DIAG was obtained and a final kissing-balloon inflation was performed (Video 3).
Final angiographic and IVUS evaluation confirmed the successful stenting of the DIAG, and that the LAD was not jeopardized and remained free of significant disease, with a minimal lumen area at the polygon of confluence (POC) > 8 mm2 (Video 4, Figure 4).
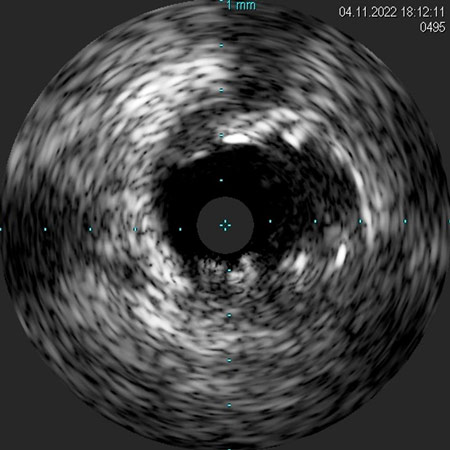
Figure 4: IVUS pullback from the LAD showing the final result of the stent implantation at the polygon of confluence (POC) of the DIAG and the LAD.
Final remarks
This case highlights the possibility of safely performing the first half of the DK-crush technique to secure, with DES implantation, the side branch of a true 0,0,1 bifurcation lesion, while avoiding the subsequent steps if stenting of the main vessel is deemed unnecessary.
Original tweet and Twitter discussion
ACS. IVUS confirmed 0,0,1 LAD/D1 bifurcation. How would approach? 2 or 1 DES or DEB? #radialfirst#cardiotwitter#PCIcase@mmamas1973@mirvatalasnag@LAzzaliniMD@GoranEBC@BURZOTTA_F@ItaloPorto2@gbiondizoccai@DrAmirKaki@PCRonline@SABOURETCardio@EmanueleBarba13pic.twitter.com/ewjULzpwqJ
— Giuseppe Andò (@giuseppe_ando) November 4, 2022
Authors


3 comments
Excellent. Why did you do 2 kissings as you did only 1st half of DK crush?
@Mahmoud Elrayes: thank you for commenting. Actually, the first kissing inflation may be considered redundant as it was finalized at optimizing DIAG ostium before crushing more proximal struts.
Thank you for commenting. Actually the first kissing inflation that was done might be considered redundant, as the aim was to optimize DIAG ostium stent expansion.