09 Feb 2023
The effect of eliminating the hydrostatic pressure gradient during fractional flow reserve measurement
Supported by the EuroIntervention Journal
Study the case of this 78-year-old male patient to understand why and how HPG may be important when measuring FFR in patients with CAD, as its height may influence the height of different FFR measurements, and, therefore, the patient management.
Authors
Rob Eerdekens MD MSc1, Mohamed El Farissi MD1, Koen Teeuwen MD PhD1, Pim A.L. Tonino MD PhD1, Lokien X. van Nunen MD PhD2
Introduction
The effect of the hydrostatic pressure gradient (HPG) on fractional flow reserve (FFR) measurements can be of varying importance in different coronary arteries. The HPG could have a significant impact when measuring FFR with traditional sensor-tipped wires, where the HPG is not eliminated.
However, as in this case, the new open-wire technology eliminates the HPG and results in different FFR, which may have clinical significance. This case illustrates the effect of HPG on FFR in the left main coronary artery with (traditional sensor-tipped wire) and without (open-wire technology) the effect of HPG.
Case summary
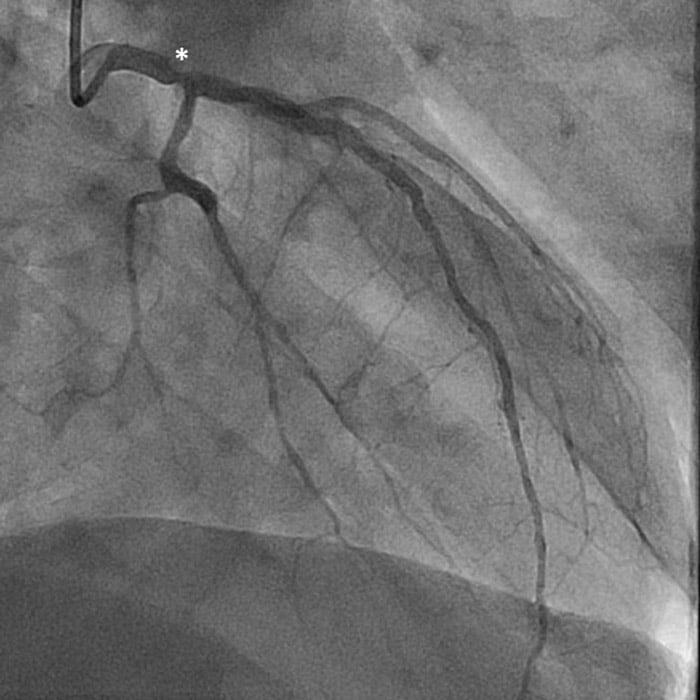
A 78-year-old male patient, with a history of percutaneous coronary intervention (PCI) of the right coronary artery (RCA) and left anterior descending coronary artery (LAD), underwent coronary angiography for long-lasting and persistent chest pain, and a dubious myocardial perfusion scintigraphy. Coronary angiography revealed haemodynamically insignificant intra-stent restenosis of the RCA, and an intermediate left main stenosis (Figure 1).
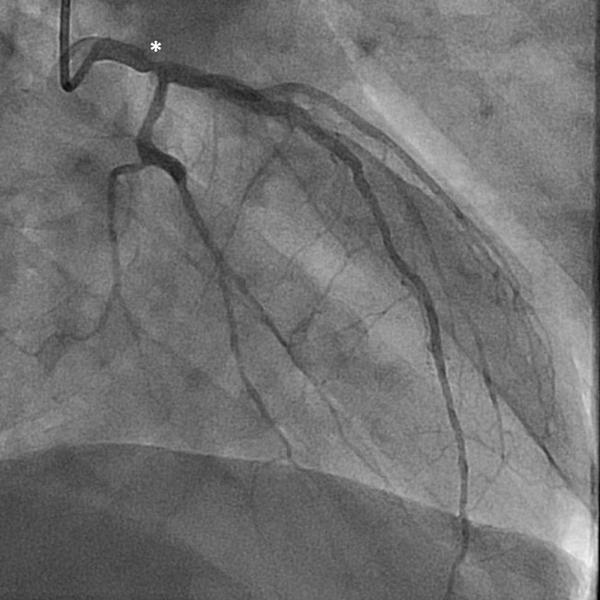
Figure 1. Diagnostic coronary angiogram, revealing an intermediate left main stenosis (white asterisk).
To assess the hemodynamic significance of this intermediate stenosis, FFR-measurement was performed, using continuous infusion of adenosine (140 µg/kg/min) and the PressureWire X® (Abbott Medical) sensor-tipped, positioned in the mid-segment of the LAD. At this position, FFR was 0.78, with a gradual increase in Pd during pullback, with a small focal step-up in the left main coronary artery.
However, due to the height difference of approximately 44 mm between the guiding catheter opening and the pressure sensor (Figure 2), the resulting hydrostatic pressure gradient (HPG) might influence decision making in this case.
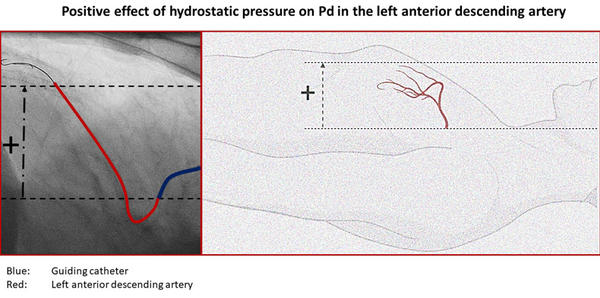
Figure 2. Left lateral fluoroscopic view at 90 degrees in order to adequately assess the height difference between the two pressure sensors in the mid LAD (red) and opening of the guiding catheter (blue). The height difference measured with angio tool was 44 mm.
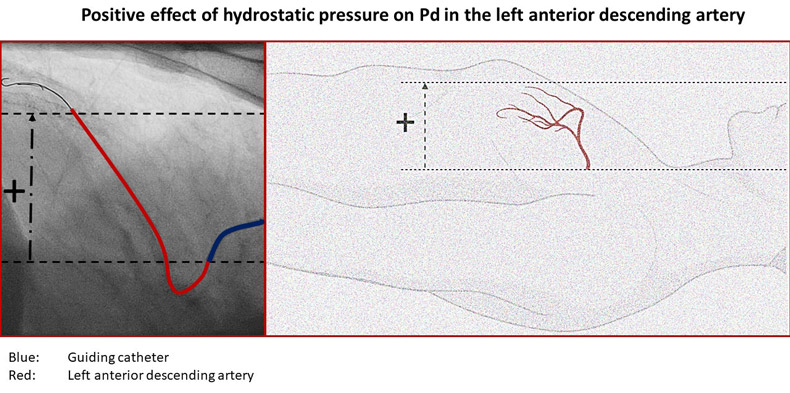
Based on the data from Härle et al., the hydrostatic pressure gradient was estimated to (falsely) decrease distal coronary pressure (Pd) by 3.4 mmHg (0.77 (factor) x 4.4 cm (height)), resulting in a lower FFR with the sensor-tipped wire.
To eliminate the effect of the hydrostatic pressure gradient, a simultaneous FFR measurement was performed, using the new Wirecath® (Cavis Technologies) with open-wire technology (per definition not affected by height differences). Simultaneous FFR measurement with the Wirecath® revealed an HPG-free FFR of 0.83, i.e. non-significant (Figure 3).
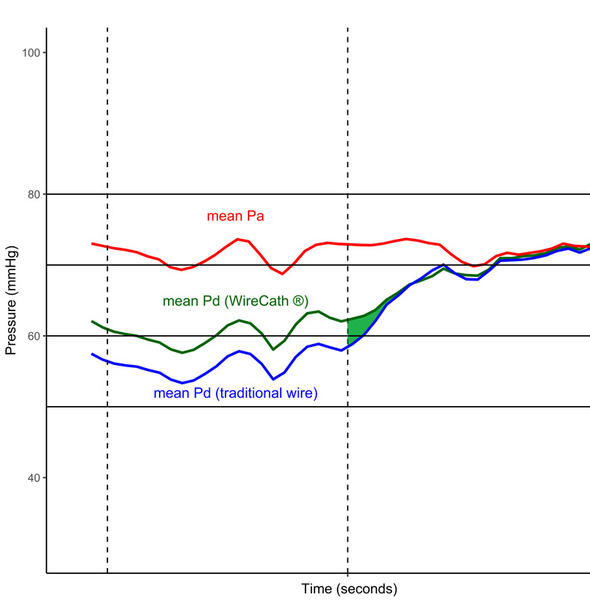
Figure 3. Simultaneous fractional flow reserve measurements (FFR) in the left anterior descending in a patient with left main stem stenosis using the PressureWire X® and Wirecath®
Pressure recordings of proximal and distal mean arterial pressure during maximal hyperemia and the simultaneous pullback (blue line: Pd measured by PressureWire X® ; green line: Pd measured by Wirecath®; red line: Pa). The shaded green segment indicates the disappearing hydrostatic pressure gradient; left dotted line: maximal hyperemia; right dotted line: start pullback. FFR with PressureWire X®0.78 was and with Wirecath® 0.83.
When performing a simultaneous pullback recording, the disappearance of the hydrostatic pressure gradient (due to the slow equalization of the height between pressure sensor and the guiding catheter opening by pulling back the pressure guidewires) can be appreciated. No drift was observed with either pressure guide.
The new Wirecath® pressure guidewire is currently being studied in the ongoing PW-COMPARE study (NCT04802681). This study will provide clear insight into the magnitude and importance of the hydrostatic pressure gradient.
Additional videos
Discussion
The HPG can be significant in patients with coronary artery disease, when measuring FFR. The height of this gradient can affect the height of the FFR measurements, and can therefore affect patient management, as in this case.
How patient outcome is affected by this open-wire needs to be studied in a larger cohort. This study is currently ongoing (NCT04802681).
Conclusion
The HPG can influence the height of different FFR measurements. Open-wire technology can eliminate this gradient.
Reference
- Härle T, Luz M, Meyer S, Kronberg K, Nickau B, Escaned J. Effect of Coronary Anatomy and Hydrostatic Pressure on Intracoronary Indices of Stenosis Severity. JACC Cardiovasc Interv. 2017;10:764–7
Affiliations
- Heart Center, Catharina Hospital, Michelangelolaan 2, 5623 EJ, Eindhoven, The Netherlands.
- Department of Cardiology, Radboud University Medical Center, Geert Grooteplein Zuid 10, 6525 GA, Nijmegen, The Netherlands.
Conflict of interest statement
The authors have no conflicts of interest to declare in relation to the content of this article.
2 comments
Nice case. The effect of HPG is large in this case due to the low aortic pressure, in the same way as in diastolic indices, since pressure is low in diastole.
Indeed, there is more pronounced effect of the hydrostatic pressure on the FFR in the case of lower aortic pressure. However, we calculated the average impact of hydrostatic pressure on the FFR measurements in various coronary segments assuming an aortic pressure of 100mmHg, and only a slightly lower average difference value of 0.0355 was found caused by the hydrostatic error when the piezo-electric sensor is in the mid-LAD: https://link.springer.com/article/10.1007/s10554-020-01971-w/figures/4 In the present case the distal pressure was measured to be 55 mmHg by piezo-electric sensor, while as was predicted by the height difference determined from the lateral view, the Cavis “open wire” pressure measurement showed by 3.4 mmHg higher value. Because of the 70 mmHg aortic pressure, the FFR without hydrostatic pressure increased by 0.05. It could be important to recognize that the hydrostatic pressure error has even more effect on pressure derived CFR calculation than on the hyperemic or non-hyperemic pressure ratios: https://www.mdpi.com/2075-4426/12/5/780