Hybrid step-by-step approach to perform a Robotic DK Crush PCI
Supported by the EuroIntervention Journal
View the case of this 65-year-old male patient who was staged for R-PCI of a Medina 1,1,1 distal left main lesion, and discover how the authors used a hybrid robotic and manual approach to perform a DK crush procedure using the second-generation R-PCI device.
Authors
Arif A Khokhar1,2, Aleksander Zelias3, Francesco Giannini4, Adriana Zlahoda-Huzior2,5, Dariusz Dudek4,6
Case summary
Robotic-assisted percutaneous coronary interventions (R-PCI) represent a new frontier for interventional cardiology1. As device technology and operator experience evolve, R-PCI is increasingly being used to treat more complex lesions2.
Bifurcation lesions requiring two-stent technique represent a challenge for current generation R-PCI devices due to the inability to actively control multiple wires and devices simultaneously.
To overcome this limitation, we describe our hybrid robotic and manual approach to perform a double-kissing (DK) crush procedure, using the second-generation CorPathGRX (Corindus, USA) R-PCI device.65-year-old male patient was staged for R-PCI of a Medina 1,1,1 distal left main lesion (Supplementary Video 1). Following manual cannulation with a 7Fr EBU 3.75 guiding catheter, the robotic cassette was connected with a coronary guidewire and a 3.5 x 15 mm non-compliant balloon loaded into the active wire, and device drives respectively.
An additional coronary guidewire and 3.5 x 15 mm balloon were parked in the passive drive (Figure 1). A pre-procedural plan was formulated in order to minimise the number of wire and device exchanges required within the robotic cassette. A hybrid strategy was adopted, combining robotic and manual control to perform the individual steps required for a DK crush PCI3 (Figure 2).
Figure 1: The device cassette of the CorPath GRX (Corindus Vascular Inc, USA) R-PCI system. (A) The active wire drive (red arrow) and active device drive (yellow arrow) allow for a single wire and device (balloon or stent) to be controlled robotically, with the passive drive (blue arrow) used to store multiple additional wires and/or devices. (B) For the hybrid DK Crush approach, the cassette was initially prepared with the side-branch circumflex wire (red arrow) and pre-dilatation balloon (yellow arrow) loaded into the active wire and device drives respectively with the main branch LAD wire and pre-dilatation balloon loaded in the passive drive (blue arrow)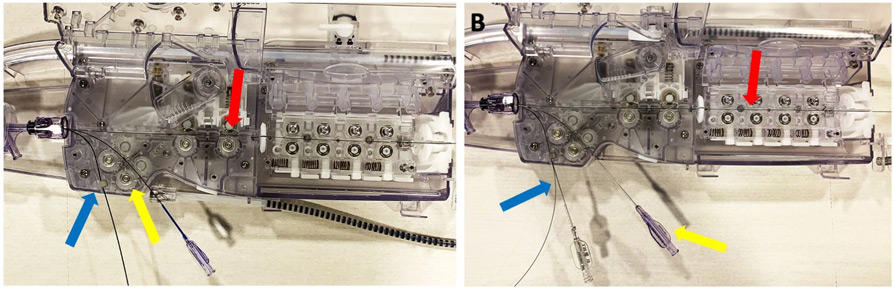
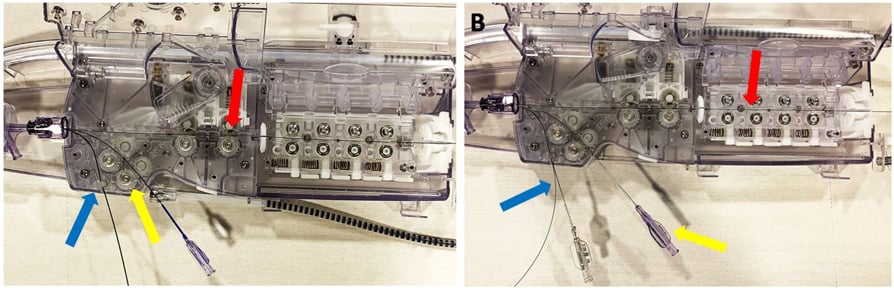
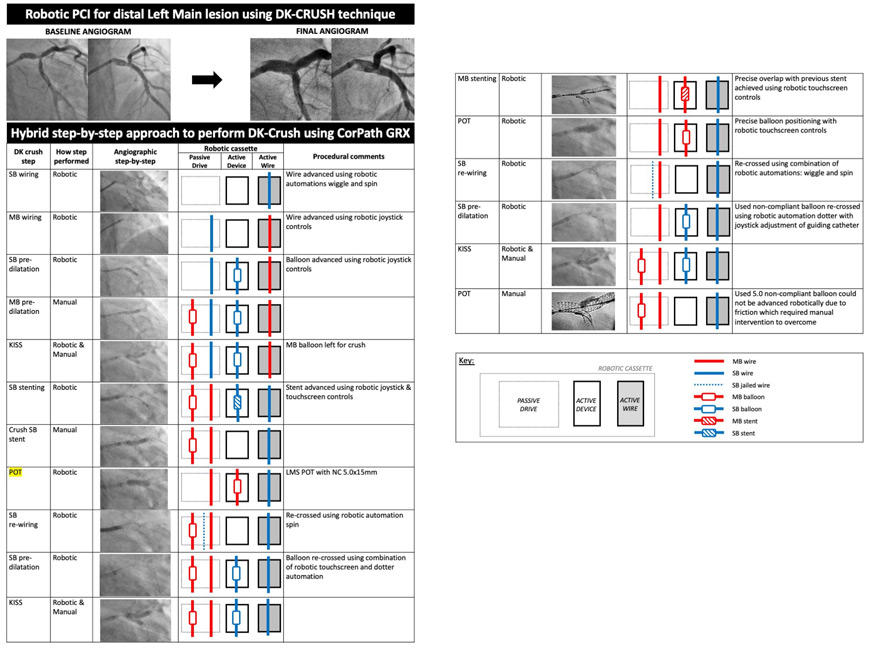
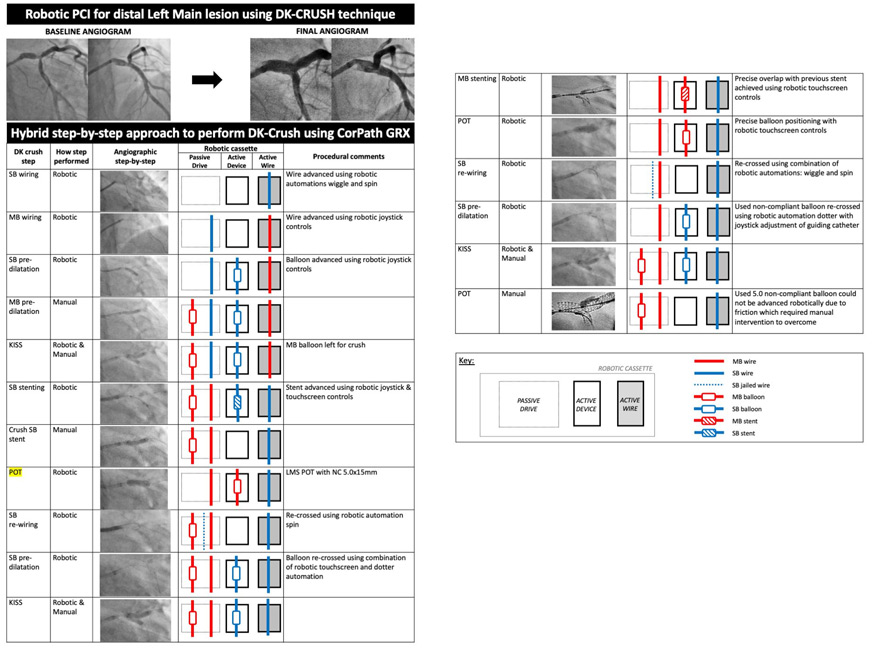
Figure 2:
Hybrid step-by-step approach for DK Crush PCI with second-generation CorPath GRX robotic platform. Step-by-step workflow demonstrating how to perform each of the recommended steps of a DK crush PCI, whilst managing the exchange of wires (solid lines), balloons (open box) and stents (crossed box) for both the main branch (red) and side branch (blue).
Side-branch interventions, re-crossing maneuvers and stent implantation were all performed under robotic control. Wire and balloon re-crossing was facilitated using the automation techniques (TechnIQTM) spin and dotter respectively. (Supplementary Videos 2 and 3).
Challenging side branch wiring, including re-crossing of stent struts, was achieved by using different combinations of the robotic wiring controls. These included joystick or 1 mm-touchscreen controls with or without the automation techniques. Use of the 1 mm touchscreen instead of joystick controls allowed for greater precision, as required during proximal cell re-wiring or balloon and stent positioning. (Figure 3)
Figure 3: (A) Touchscreen controls (red box) compared to the joystick allow the operator to perform finer (1mm) movements of either the guidewire or device. This feature facilitates accurate stent implantation and (B) precise placement of the final proximal optimisation technique balloon.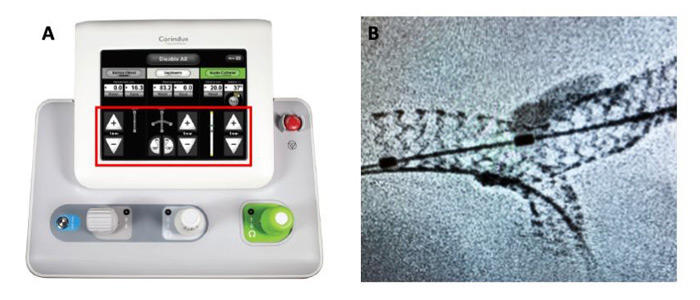
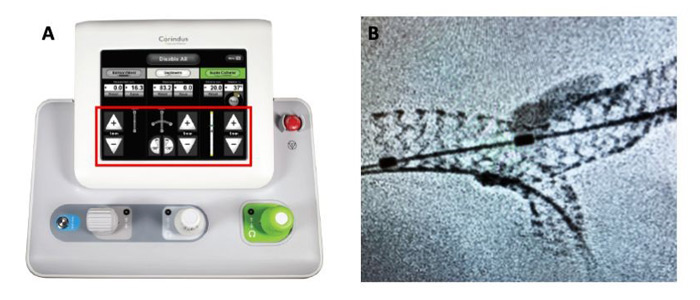
Manual control was required for main-branch and kissing and proximal optimisation technique (POT) inflations due to the inability to actively control multiple wires and devices from the robotic console. Additionally, the resistance frequently encountered during bifurcation PCI, particularly when using multiple balloons and wires, could not be overcome robotically.
If the robotic system encounters resistance during device advancement a visual alert and alarm mechanism is triggered, which prevents further advancement of the device.
→ This scenario was encountered when trying to advance a non-compliant 5.0. mm balloon for the final POT inflation and manual input was required to overcome the resistive forces.
A visual alert and alarm is triggered, which prevents further advancement of the balloon or stent and required manual intervention.
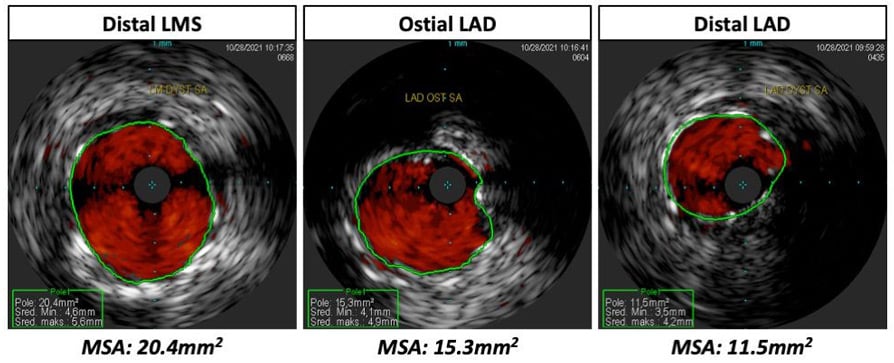
An optimal final angiographic result was achieved and confirmed by intravascular imaging (Figure 4), which did not reveal any complications. Total contrast volume was 150 mls, fluoroscopy time 35 minutes, and total radiation dose 1154 mGy. Our hybrid R-DKC procedure was possible due to the passive drive in the robotic cassette, which allows multiple wires and devices to be stored and manipulated (Figure 3).
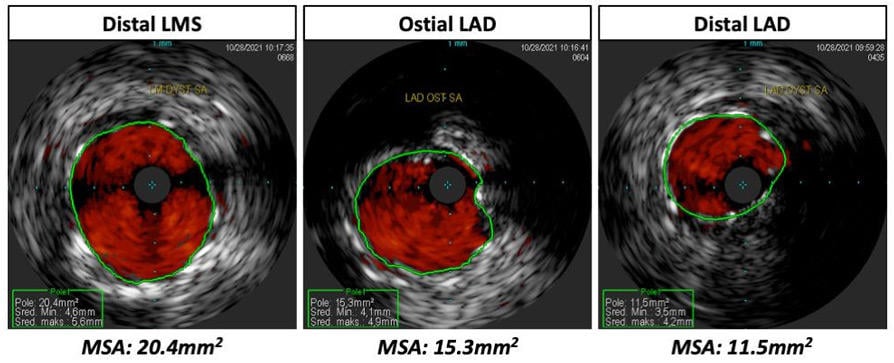
Figure 4:
Post-procedural IVUS confirmed the good angiographic result observed with (A) distal left main Minimum Stent Area (MSA) being 20.4mm2 (B) proximal LAD MSA 15.3mm2 and (C) distal LAD MSA 11.5mm2
Additionally, a device can be robotically advanced on a wire stored in the passive drive. By determining the optimal sequence of wire/device exchanges and communicating these steps in real-time to the catheter lab team using audio headsets, procedural time and efficiency can be improved.
In order to perform such hybrid procedures, two operators who are in direct communication with each other are required: a robotic operator and a manual operator who is also familiar with how to handle and exchange wires and devices within the robotic cassette.
Our hybrid R-DKC step-by-step approach allows operators to use the benefits of robotic technology, such as reduction in radiation exposure, enhanced precision, and possibility for remote-stenting, whilst allowing the limitations of current generation R-PCI platforms to be overcome.
Further improvements in device technology, such as the ability to simultaneously control multiple wires and devices, will enable operators to perform increasingly more complex interventions robotically.
Supplementary Material
References
- Beyar R, Davies JE, Cook C, Dudek D, Cummins PA, Bruining N. Robotics, imaging, and artificial intelligence in the catheterisation laboratory. EuroIntervention. 2021;17:537–49.
- Mahmud E, Naghi J, Ang L, Harrison J, Behnamfar O, Pourdjabbar A, Reeves R, Patel M. Demonstration of the Safety and Feasibility of Robotically Assisted Percutaneous Coronary Intervention in Complex Coronary Lesions: Results of the CORA-PCI Study (Complex Robotically Assisted Percutaneous Coronary Intervention). JACC Cardiovasc Interv. 2017;10:1320–7.
- Hall AB, Chavez I, Garcia S, Gössl M, Poulose A, Sorajja P, Wang Y, Louvard Y, Chatzizisis YS, Banerjee S, Xenogiannis I, Burke MN, Brilakis ES. Double kissing crush bifurcation stenting: Step-by-step troubleshooting. EuroIntervention. 2021;17:E317–25.
Affiliations
- Imperial College Healthcare NHS Trust, London, UK
- Digital Innovations & Robotics Hub, Krakow, Poland
- Center for Invasive Cardiology, Electrotherapy and Angiology in Nowy Sacz, Poland
- Interventional cardiology unit, GVM Care & Research, Maria Cecilia Hospital, Cotignola, Italy
- AGH University of Science and Technology, Department of Measurement and Electronics, Krakow, Poland
- Institute of Cardiology, Jagiellonian University Medical College, Krakow, Poland

No comments yet!