14 Dec 2020
Three-dimensional optical coherence tomography-guided double kissing crush stenting
Supported by the EuroIntervention Journal
The authors present a case of percutaneous coronary intervention for bifurcation lesion in a 73-year-old man suffering from effort angina, in which they successfully performed double kissing crush stenting using optical coherence tomography.
Authors
Kazumasa Kurogi1, Masanobu Ishii1, Kenichi Tsujita2, Nobuyasu Yamamoto1
Case summary
We present a case of percutaneous coronary intervention for bifurcation lesion in a 73-year-old man suffering from effort angina, in which we successfully performed double kissing (DK) crush stenting using optical coherence tomography (OCT) (Abbott Vascular, Santa Clare, CA).
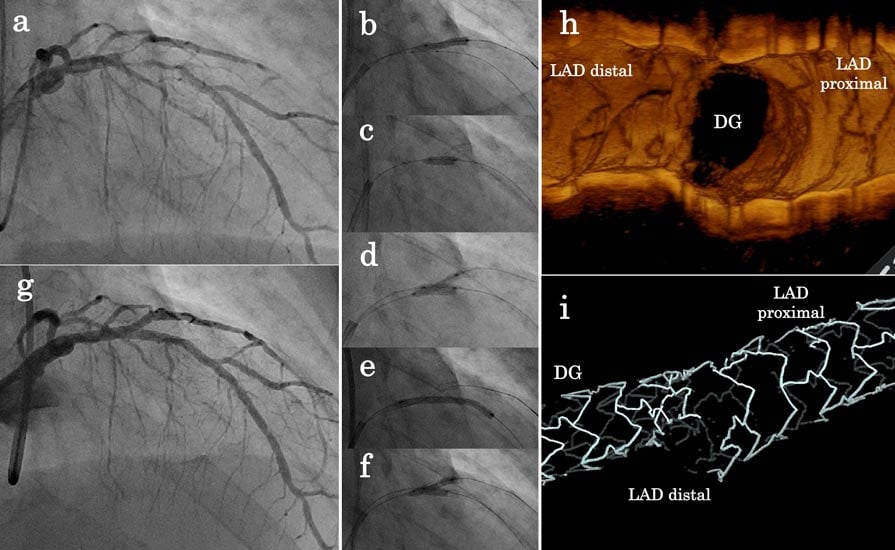
Figure 1. Angiography and the three-dimensional optical coherence tomography findings.
(a) Control angiography (b) Stenting the side branch (c) Crushing side branch stent (d) 1st kissing balloon inflation (e) Stenting main branch (f) Final kissing balloon inflation (g) Final angiography (h) Three-dimensional optical coherence tomography observing side branch ostium after final kissing balloon inflation (i) Three-dimensional optical coherence tomography pullback from the DG branch.
Coronary angiography revealed a bifurcation lesion (Medina classification: 0,1,1) (Fig. 1a, Supplement 1).
A Xience Alpine everolimus-eluting stent (2.25 x 15 mm, Abbott Vascular, Santa Clare, CA) was implanted in the diagonal branch (DG) with protrusion into the LAD (Fig. 1b) and the DG stent was crushed (Fig. 1c).
3D OCT revealed central rewiring of the guidewire and complete jailing of the DG ostium in the crushed stent (Supplement 2).
After the first kissing balloon inflation (KBI) (Fig. 1d), imaging revealed successful removal of stent struts from the DG ostium (Supplement 3).
A Xience Alpine everolimus-eluting stent (3.5 x 28 mm) was implanted in the LAD (Fig. 1e). 3D OCT showed excellent stent expansion and coverage of the DG ostium (Fig. 1h,i and Supplement 4) after the final KBI (Figure 1f).
Final angiography showed good result (Fig. 1g, Supplement 5).
Crush stenting generates multiple layers of stent struts covering the side branch (SB) and causes difficult guidewire re-crossing [1].
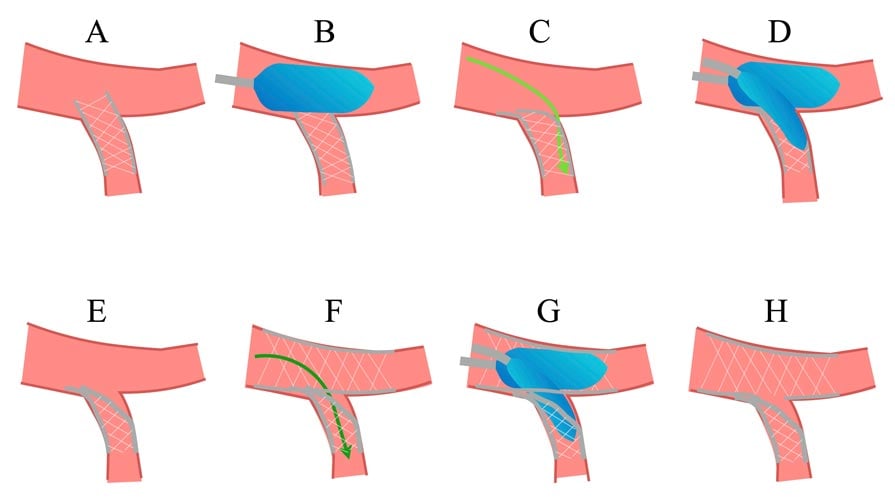
DK crush stenting reduces the strut layer in the SB ostium and facilitates the final KBI, which results in favourable clinical outcomes [2]. However, there is a possibility of suboptimal DK crush stenting in the conventional method (Supplement 6, A-H); if the SB guidewire passes the wrong strut (Supplement 6, C), stent deformation could occur after the first KBI (Supplement 6, E).
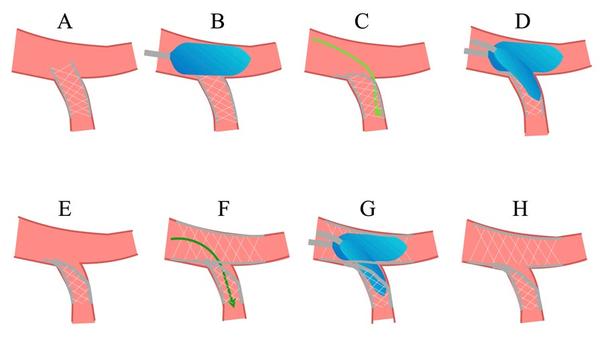
Supplement 6. Figure for explanation; Suboptimal double kissing crush stenting
3D OCT imaging allows observations of the crushed SB stent strut and the guidewire re-crossing point before the first KBI. Moreover, 3D OCT allows confirmation of the guidewire re-crossing point before the final KBI. 3D OCT could optimize DK crush stenting for bifurcation lesions.
Conflict of interest statement
Dr. Tsujita has received remuneration for lecture from Amgen Astellas BioPharma K.K., Kowa Pharmaceutical Co. Ltd., Daiichi Sankyo Co., Ltd., Takeda Pharmaceutical Co., Ltd., Bayer Yakuhin, Ltd., Pfizer Japan Inc., Bristol-Myers K.K., MSD K.K.; has received trust research/joint research funds from Bristol-Myers K.K., Sugi Bee Garden Co., Ltd., Kowa Pharmaceutical Co. Ltd.; and has received scholarship fund from ITI Co., Ltd., Abbott Medical Japan L.L.C, Abbott Vascular Japan Co., Ltd., Otsuka Pharmaceutical Co., Ltd., Cardinal Health Japan, Kaneka Medix Co., Ltd., Takeda Pharmaceutical Co., Ltd., Mitsubishi Tanabe Pharma, Chugai Pharmaceutical Co., Ltd., TERUMO Co., Ltd., NIPRO CORPORATION, NIHON KOHDEN CORPORATION, Medtronic Japan Co., Ltd., Japan Lifeline Co., Ltd., Fides-One, Inc., Fukuda Denshi Co., Ltd., and Boston Scientific Japan K.K.
All the other authors have nothing to disclose.
Affiliations
- Department of Cardiovascular Center, Miyazaki Prefectural Nobeoka Hospital, Nobeoka, Japan
- Department of Cardiovascular Medicine, Graduate School of Medical Sciences, Kumamoto University, Kumamoto, Japan
References
- Ormiston JA, Webster MW, Webber B, Stewart JT, Ruygrok PN, Hatrick RI. The "crush" technique for coronary artery bifurcation stenting: insights from micro-computed tomographic imaging of bench deployments. JACC Cardiovasc Interv 2008; 1:351-357.
- Chen SL, Zhang JJ, Han Y, Kan J, Chen L, Qiu C, Jiang T, Tao L, Zeng H, Li L, Xia Y, Gao C, Santoso T, Paiboon C, Wang Y, Kwan TW, Ye F, Tian N, Liu Z, Lin S, Lu C, Wen S, Hong L, Zhang Q, Sheiban I, Xu Y, Wang L, Rab TS, Li Z, Cheng G, Cui L, Leon MB, Stone GW. Double Kissing Crush Versus Provisional Stenting for Left Main Distal Bifurcation Lesions: DKCRUSH-V Randomized Trial. J Am Coll Cardiol 2017; 70:2605-2617.

1 comment
Without the help of OCT and IVUS, how to ensure entry of guide wire into side branch at right point ?