17 Mar 2021
Overcoming the 360 degree radial artery loop
Supported by the EuroIntervention Journal
A 77-year-old man was admitted for an elective diagnostic coronary angiogram. Following insertion of a 6Fr sheath into the distal right radial artery, a radial angiogram showed complete 360 degree radial artery loop...
Authors
Karthick Manoharan1, Pitt O Lim1
Case summary
A 77-year-old man was admitted for an elective diagnostic coronary angiogram. He had CABG in 2012 and has had multiple coronary interventions over the past 2 years for graft failures. Previous right radial access was unsuccessful because of difficulty in advancing any catheter beyond the elbow, likely to be due to wiring of the straight but small radial recurrent artery, now with hindsight (Panel A). Prior left radial approach was hindered by left subclavian artery tortuosity and a kinked catheter, and femoral access was complicated by significant groin haematoma.
On this occasion, following insertion of a 6Fr sheath into the distal right radial artery, a radial angiogram was performed upfront which showed a complete 360 degree radial artery (loop). Under normal circumstances, an alternative access site should be sought, as straightening such a loop is painful “if it could be done at all” and catheter exchanges would be traumatic and difficult, if not impossible. However, in view of the above experiences, we decided to persist with the strategy described below which has not been tested in the past.
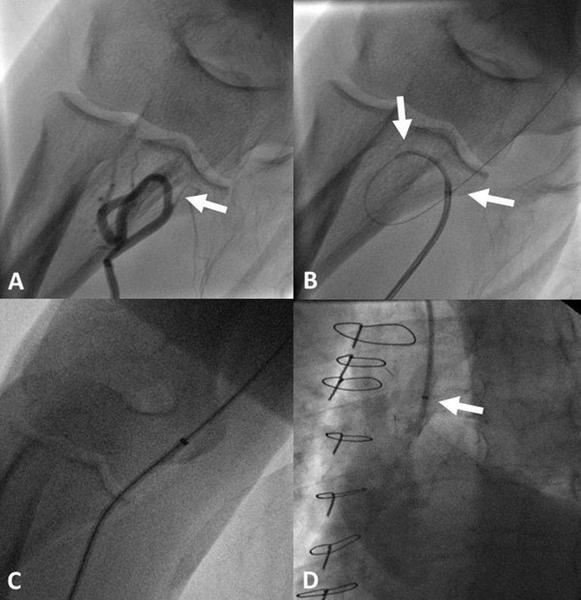
Panel A - 360 degree radial loop and radial recurrent artery (arrow).
Panel B - A 4Fr Pigtail catheter (left arrow) as an introducer within a 5Fr JR4 guide (right arrow) on an angioplasty wire.
Panel C - Cook’s Flexor® 6Fr 90cm hydrophilic guiding sheath with introducer traversing the straightened loop on a J-tipped 0.035” wire.
Panel D - Guiding sheath in the ascending aorta adapted with Terumo’s Radifocus® haemostatic valve turning it into an ‘extra-long’ sheath with contrast injection (arrow).
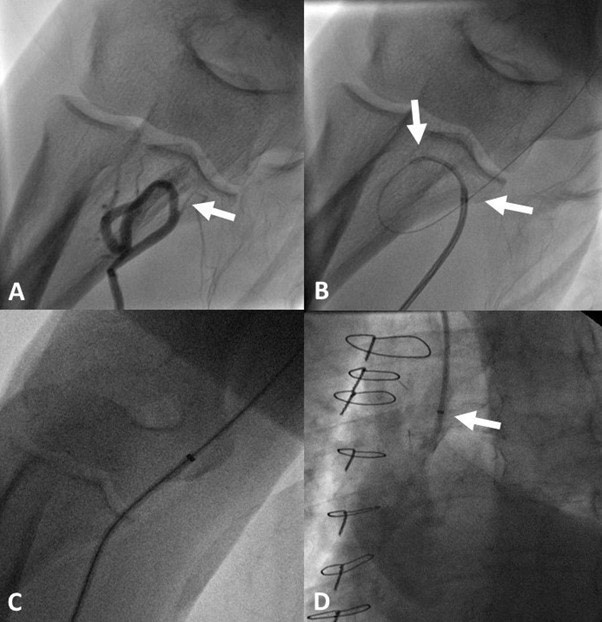
An angioplasty 0.014” guidewire was advanced down the radial artery traversing the loop into the brachial artery. A 5Fr JR4 guide was then advanced into the loop, but it failed to cross because of wire bias. To overcome this, a 4Fr Pigtail catheter was introduced into the 5Fr JR4 guide; firstly, to provide a graduated telescopic tapering tip, secondly, the tip is curved to allow the system to take the shape of the loop which overcomes the “razor tip phenomenon” (Panel B), and thirdly, it provides support to increase the pushability of the 5Fr JR4 guide. Once the system crossed the loop, it was twisted anticlockwise to straighten the loop, and this allowed the system to be advanced into the aorta. Next, a J-tipped 0.035” 260 cm exchange length wire was inserted with the tip parked in the aortic root, and then the catheters were removed.
Finally, a 6Fr 90 cm hydrophilic guiding sheath (Cook Medical, Bloomington, IN, USA) was pushed across the straightened loop (Panel C) into the ascending aorta, and a short haemostatic valve (Terumo Corporation, Tokyo, Japan) was attached to the other end turning this into an 'extra-long' sheath to allow painless and seamless multiple catheter exchanges to complete the procedure.
Conflict of interest statement
The authors have no conflict of interest to declare.
Affiliation
- Department of Cardiology, St George’s Hospital, London, UK
3 comments
Thank you for sharing. In my practice I straightened a 360 degree loop twice . One by using a hydrophilic Terumo wire and the other I needed a Pilot 50 PCI wire (I just didn’t think it’s something to be shared though your idea of using telescopic catheters including a pigtail was brilliant) Amjad Almendilawi, Baghdad, Iraq
Overcoming loops or komplex bifurcations of the fore or upper arm is one of the radialist’s challenges. Thank you for the presentation. Nice example and interesting solution! However, at least for radially experienced there maybe a more simple way - especially in cases with such a big loop radius: Just keep the 35 workhorse (nonhydrophilic) wire, put the catheter (not necessarily pigtail) on and bring it to the beginning of the loop which will provide better support. Then lead the railed 35 wire forward carefully - (at first) without moving the catheter. Then also move cath under slightly twisting it so the vessels geometry changes and may help passing the loop - less time consuming, without (or hardly) extra material, easier and last not least still nontraumatic. Christoph Langer, Bremen, Germany
Overcoming loops or komplex bifurcations of the fore or upper arm is one of the radialist’s challenges. Thank you for the presentation. Nice example and interesting solution! However, at least for radially experienced there maybe a more simple way - especially in cases with such a big loop radius: Just keep the 35 workhorse (nonhydrophilic) wire, put the catheter (not necessarily pigtail) on and bring it to the beginning of the loop which will provide better support. Then lead the railed 35 wire forward carefully - (at first) without moving the catheter. Then also move cath under slightly twisting it so the vessels geometry changes and may help passing the loop - less time consuming, without (or hardly) extra material, easier and last not least still nontraumatic. Christoph Langer, Bremen, Germany