Comparison of stent geometry achieved by different side-branch ballooning techniques for bifurcation provisional stenting: the CRABBIS Trial
Selected in JACC: Cardiovascular Interventions by A. Nazmi Calik , A. Cader
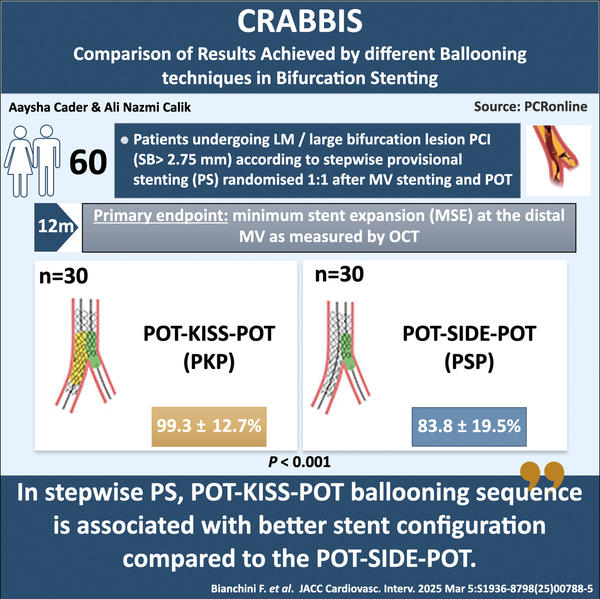
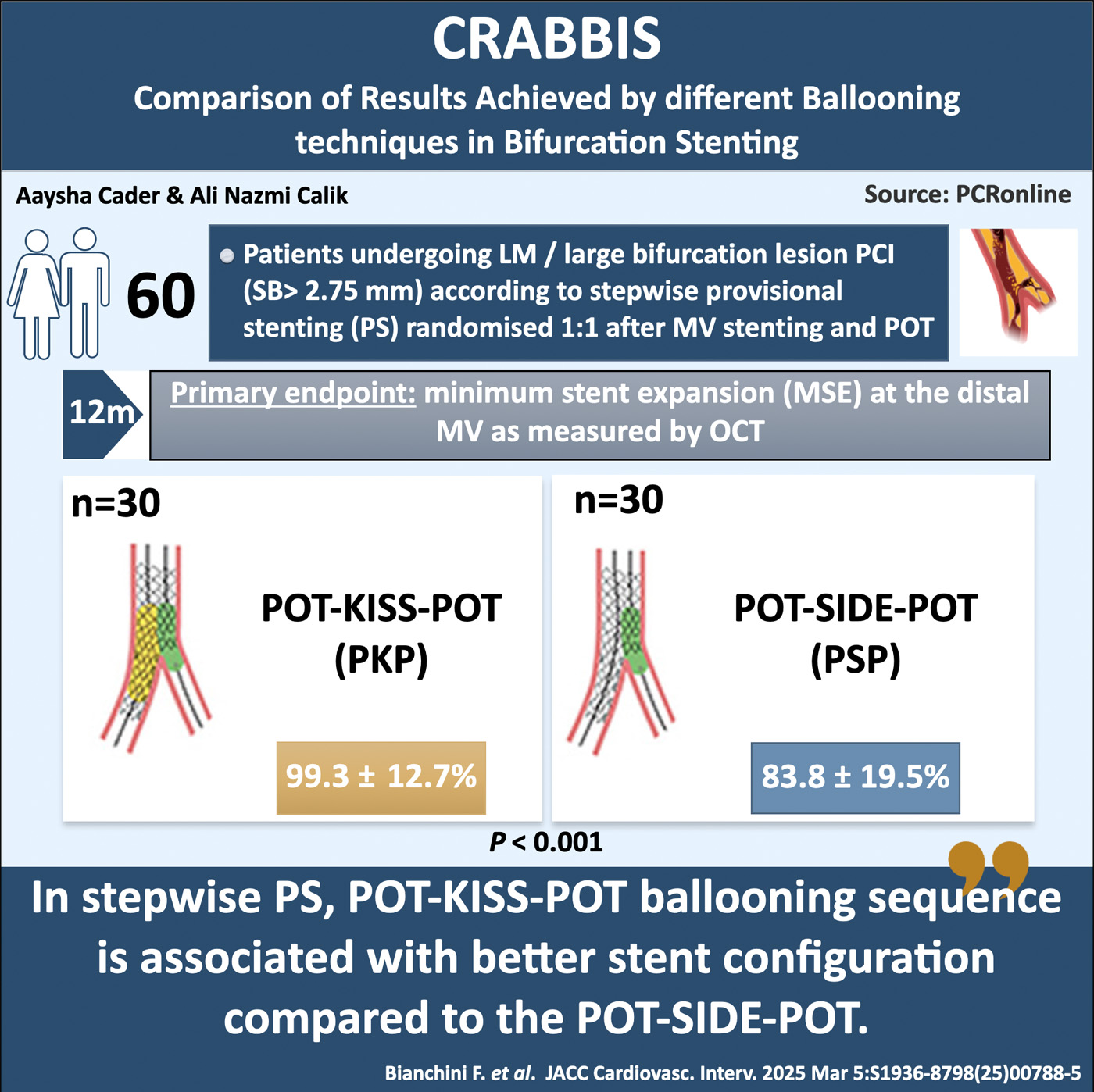
Which ballooning technique is best after main vessel stenting in bifurcation PCI? This two-part study compares two key approaches: PKP (POT, kissing balloon inflation, final POT) and PSP (POT, isolated side branch dilation, final POT) to determine the optimal strategy.
References
Authors
Francesco Bianchini, Enrico Romagnoli, Cristina Aurigemma, Lazzaro Paraggio, Antonino Buffon, Francesco Fracassi, Mattia Lunardi, Luigi Cappannoli, Emiliano Bianchini, Andrea Zito, Carlo Trani, and Francesco Burzotta
Reference
J Am Coll Cardiol Intv. Mar 10, 2025. Epublished DOI: 10.1016/j.jcin.2025.02.007
Published
2025 Mar, 10
Link
Read the abstractReviewers


Our Comment
Designed by Aaysha Cader & Ali Nazmik Calik. Source: PCRonline.com
Why this study – the rationale/objective?
A stepwise provisional strategy (PS) is the recommended approach for contemporary coronary bifurcation lesion (CBL) percutaneous coronary interventions (PCI)1. Crossover stenting in the main vessel (MV) followed by post-dilation of the proximal stented segment (proximal optimisation technique, [POT]) are essential steps of PS.
After MV stenting, there are two main techniques for side branch (SB) ballooning sequences:
- Proximal-optimisation-technique (POT)+kissing-balloon inflation+ final POT (PKP).
- And POT+isolated-SB-dilation+final POT (PSP).
The best technique for ballooning remains debated. This question was addressed in a two-part research project.
How was it executed – the methodology?
- Pre-clinical trial: undertaken in non-atherosclerotic animal coronary models at Visible heart® Lab, this study found that:
- PSP was more effective in preserving stent circularity at the proximal MV segment;
- PKP provided better stent expansion at the distal MV and higher SB scaffolding at the polygon of confluence2
- RCT: The CRABBIS trial (Comparison of Results Achieved by different Ballooning techniques in Bifurcation Stenting; NCT05559424): an open-label, prospective, randomised, single-centre trial aimed to compare bifurcation PCI stent configurations outcomes (by OCT, performed with either PSP vs PKP (randomised 1:1)3.
Inclusion criteria:
De novo CBL involving either the left main (LM) bifurcation or large branch non-LM (SB diameter > 2.75 mm and distal MV reference diameter ≥ 3.5 mm) bifurcations were recruited, including all Medina lesions, except Medina 0.0.1. The MV stent was implanted over the MV in crossover to the SB, followed by POT (balloon sized 1:1 to proximal MV reference diameter), placing the distal marker just proximal to the carina. Patients were then randomised 1:1 to either PKP or PSP, after successful MV stenting and POT.
PKP arm: SB rewiring by pullback technique, KBI (short balloons, MV balloon sized 1:1 to distal MV and SB balloon sized 1:1 to SB diameters)(4) and final POT in typical fashion
PSP arm: SB rewiring (as in PKP), SB dilatation (balloon sized 1:1 to SB reference diameter) with minimal balloon protrusion into proximal MV, then final POT
Post-stenting OCT undertaken, representing the “index” OCT for study comparisons. Stent configuration (i.e. expansion, apposition and eccentricity) at five different bifurcation segments
were defined and measurements recorded, with reference lumen area for each segment appropriately defined according to proximal and distal MV.
Endpoints:
Primary endpoint was minimum stent expansion (MSE) at the distal MV. MSE was expressed in percentage as the ratio between minimal stent cross-sectional area (CSA) in each sub-segment and the corresponding reference lumen area.
Secondary endpoints were MSE in other segments, maximum distance and area of malposition, Stent Eccentricity Index (SEI) and SB scaffolding length.
What is the main result?
A total of 60 patients undergoing stepwise provisional bifurcation PCI were randomised 1:1 to either PKP vs PSP4. Baseline clinical characteristics were similar between groups, representing a low clinical risk population. Mean age was 70.3 ± 9.4 years. Chronic coronary syndrome was 53.3 % vs 70 % for PKP vs PSP. No significant differences for baseline angio characteristics: majority of PCI were LM interventions (86.7 % vs 83.3 % in PKP vs PSP). Medina 1,1,1 lesions were 23.3 % vs 26.7 % for PKP vs PSP respectively. Baseline OCT characteristics showed no difference in plaque composition between the two arms. Radial approach was predominantly used > 93.3 % in both arms and MV predilatation was done in 100 % of both arms. There were no differences in MV stent diameters and lengths, POT balloons or SB balloon diameters and lengths used for either PKP or PSP.
MSE: The primary endpoint, MSE at the distal MV segment was significantly higher with PKP as compared with PSP (99.3 ± 12.7 % vs. 83.8 ± 19.5 %; p < 0.001). There was also higher MSE at the bifurcation core, but no differences un MSE in the proximal MV segments.
There were no significant differences in lumen areas and stent areas between the PSP and PKP groups. Also, no significant differences were seen in SEI, at either the proximal MV, bifurcation core or the distal MV.
Stent apposition: PSP group showed greater malapposition distance and greater malapposition area, both in the bifurcation core (median: 0.9 [IQR: 0.2-2.3] mm2 in PSP vs. 0.2 [IQR :0.2-0.2] mm2 in PKP;p < 0.001) and in the distal MV (median:0.5 [IQR:0.2-1.0] mm2 in PSP vs.0.2 [IQR:0.1-0.2] mm2 in PKP; p<0.001).
Thus, at distal MV, the PSP approach resulted in a higher rate of major under-expansion (26.7 % vs. 3.3 %; p = 0.026) and major malapposition (50.0 % vs. 10.0 %;p < 0.001), when compared with PKP.
At the bifurcation core, PKP group was associated with a significant increase in maximal stent diameter (5.3 ± 0.9 vs. 4.7 ± 0.7 mm; p = 0.006) and SB scaffolding length (1.9 ± 0.9 vs. 1.2 ± 0.5 mm; p < 0.001). PKP also resulted in a significantly greater SB minimal lumen diameter (2.4 ± 0.6 mm vs. 2.1 ± 0.6 mm; p = 0.015), when compared with PSP. Furthermore, after the SB ballooning sequences, a significantly higher number of procedures in PSP group needed
additional treatments to address stent complications (73.3 % vs. 16.7 %; p < 0.001).
Critical reading and the relevance for clinical practice:
The main findings are:
- PKP resulted in more favourable stent configurations at the distal MV and bifurcation core, attributed to a significant higher stent expansion and lower rate of malapposition.
- At the proximal MV, PKP and PSP resulted in similar results in terms of stent expansion, apposition and eccentricity.
One of the important detrimental effects of PSP caused by isolated SB dilation is a carina-shift towards the MV, thus deforming the stented areas near the carina, leading to incomplete stent expansion and apposition at distal MV. These are not observed after KBI, as the simultaneous balloon inflation in the MV and SB helps maintain the central position of the carina.
At the bifurcation core, as the absence of kissing did not allow the stent to be stretched towards the SB, PSP resulted in shorter SB scaffolding length. Longer, good SB scaffolding found in PKP facilitates the placement of a second stent during bailout SB stenting by making a favourable configuration.
Comparable stent eccentricity was seen in the proximal MV with both PKP and PSP. Refinements of the PKP technique whereby KBI with minimal balloon overlapping in proximal MV and meticulous re-POT to re-dilate the entire proximal MV restoring circularity, may explain this, and should be the technique to be followed in PKP.
Despite the meticulous OCT measurements undertaken, this study remains one focused on stent geometry, and impact on clinical outcomes has not been assessed. Also, this was a single centre study, whereby operator expertise may also have played a role in these outcomes.
References
- Hildick-Smith D, Egred M, Banning A, et al. The European bifurcation club Left Main Coronary Stent study: a randomized comparison of stepwise provisional vs. systematic dual stenting strategies (EBC MAIN). Eur Heart J. 2021;42:3829–3839.
- Bianchini F, Cangemi S, DeVos A, et al. Multimodal Comparisons of Results Achieved by Different Side Branch Ballooning Techniques for Bifurcation Provisional Stenting. Circ Cardiovasc Interv. 2023;16:e012908
- Bianchini F, Romagnoli E, Aurigemma C, Paraggio L, Buffon A, Fracassi F, Lunardi M, Cappannoli L, Bianchini E, Zito A, Trani C, Burzotta F. Comparison of stent geometry achieved by different side-branch ballooning techniques for bifurcation provisional stenting: the CRABBIS trial. JACC Cardiovasc Interv. 2025 Mar 5:S1936-8798(25)00788-5. doi: 10.1016/j.jcin.2025.02.007. Epub ahead of print. PMID: 40071321.
- Burzotta F, Paraggio L, Aurigemma C, et al. How to perform simultaneous kissing balloon inflation with a single inflation device. PCR Online. 2023

No comments yet!