17 Apr 2020
Why and how to perform Proximal Optimisation Technique (POT)
Proximal stent optimization to pMV reference diameter needs to be performed with an adequately sized (1:1) and meticulously positioned balloon since either too proximal or too distal position of POT balloon leads to suboptimal results. Discover the tips and solutions proposed by Zlatko Mehmedbegovic et al.
Frequency of the problem:
Expert level:
Summary
Bifurcation lesions remain challenging to interventional cardiologists due to their unique fractal anatomy, which means that there is a step-down reduction in the main vessel (MV) diameter at each bifurcation site. As a result, coronary bifurcation consists of three coronary segments, proximal and distal MV (pMV and dMV) and the side branch (SB), and there is a constant relation between these 3 segments, defined by the Murray’s law, which has been simplified by Finet formula.
Because of discrepancy in diameters between the pMV and the dMV and the fact that coronary stents have a tubular design, proximal optimization technique (POT) has been proposed to “reconstruct” natural, fractal geometry of coronary bifurcation and reach adequate matching with the individual patients’ anatomy. POT represents a systematic post-dilation of the stent in the proximal MV up to the carina level with balloon sized 1:1 according to the proximal MV.
Particular attention should be paid to position the distal marker of the POT balloon in front of the carina. The main role of the POT is to achieve optimal stent expansion and apposition in the proximal segment. In addition, it opens the stent cells and creates an oblique shape in front of the SB, thus facilitating recrossing and advancement of devices through the implanted stent. Though both, semi-compliant and non-compliant balloons can be used for POT, non-compliant balloons are preferred in the presence of toughen stent under-expansion. According to European Bifurcation Club consensus documents, POT is recommended as a mandatory step of bifurcation stenting.
The problem
In provisional SB stenting strategy, stent diameter is selected according to the distal MV size in order to avoid carina shift towards the SB ostium and to avoid dMV dissection. As a drawback, stent will be “under-sized” in the pMV leading to significant stent malapposition. Stent underexpansion may have immediate implications during bifurcation PCI since an SB guidewire may unintentionally pass either behind the stent struts or “in-and-out” stent, which is not visible on angiography nor provides a “tactile feedback” to the operator. Therefore, postdilatation is important to ensure adequate vessel and stent expansion. With POT, workhorse stents can be adapted to the fractal anatomy of bifurcation lesions, especially in bifurcation lesions with a large SB, where there is a greater discrepancy between the proximal and distal MV diameters.
Proximal stent optimization to pMV reference diameter needs to be performed with an adequately sized (1:1) and meticulously positioned balloon since either too proximal or too distal position of POT balloon leads to suboptimal results.
Principal idea
The expected benefits of the POT are:
- to achieve full apposition of the stent proximal to the bifurcation and to correct underexpansion (Figures 1 and 2)
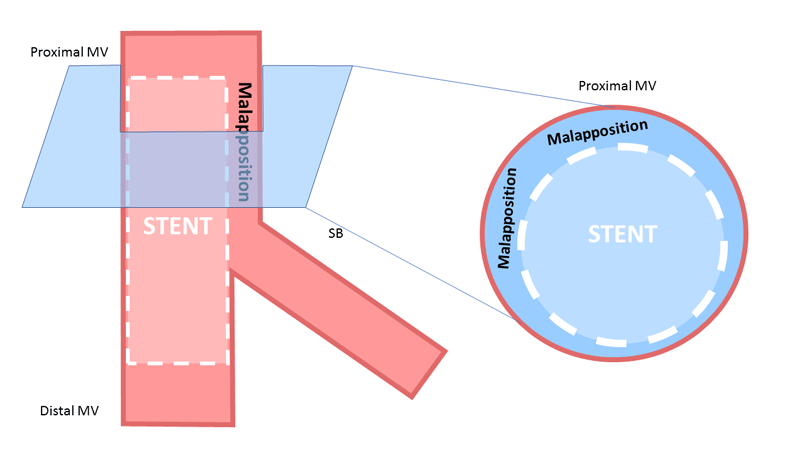
Figure 1.
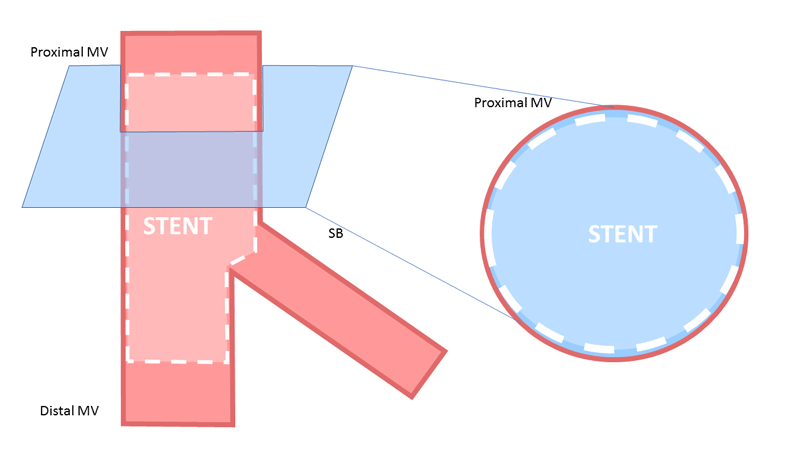
Figure 2.
- to preclude any unintended wire (or other device) passage behind stent struts
- to mediate SB rewiring by expanding the stent cells overlying the SB ostium, thereby facilitates “optimal re-cross” through distal cells
- to facilitate further access to side branch by any device used (balloon, wire, stent etc.) by pushing aside mal-apposed struts
- to correct final stent deformation following kissing balloon inflation or SB dilatation
Material needed
Short, sized 1:1 to proximal MV diameter, non-compliant (or semi-compliant) coronary balloon
Method step-by-step
- use short non-compliant or semi-compliant balloon immediately following stenting of the MV
- place distal balloon marker just above/in front of the carina level
- make sure to be in a “most orthogonal” projection to the SB take-off while positioning the balloon
- in fluoroscopy use stent enhancement software, if available, to precisely position the distal balloon marker
- use adequate balloon pressure to dilate the unopposed stent
- remember to optimize the full length of the pMV stent segment repeating the process up to the proximal stent edge (attention needed to stay with the balloon inside the stent)
Points of specific attention
- always plan bifurcation PCI procedure according to available material (shortest length of the balloon available for POT < pMV stented length), shortest available sizes on the market are 6 and 8 mm
- read balloon specifications used for POT (differ among manufacturers), like a “shoulder” length, compliance chart, etc.
- never force and push balloon to avoid stent deformation, especially prior to performing POT
- balloon position for final POT/re-POT needs to be intentionally performed more “proximal” to first POT (especially after stenting both branches with newly formed metallic neocarina, eg. TAP)
- in case of large pMV segments, semi-compliant balloons could be advantageous to non-compliant due to the greater expansion range, while non-compliant are preferred in case of stent underexpansion
A word from the reviewer - Julien Adjedj
POT, is the key technique which makes bifurcation PCI safer and easier.
The POT balloon positioning is of importance in this technique, protecting the side branch with another wire will allow:
- To find the best projection to align the distal marker of the POT balloon to the carina.
- To facilitate balloon positioning
- To bring more support and open narrow bifurcation angles
- To protect the side branch.
The balloon diameter is of importance to obtain optimal stent apposition in the main branch. A practical sign is to administrate a small amount of contrast medium (puff) during POT balloon inflation:
- If contrast medium progresses through the balloon, operator might suspect stent malapposition in the proximal main vessel
- If contrast medium progression is stopped at the proximal part of the POT balloon, it is likely to have good stent apposition in the proximal main vessel.

Authors


4 comments
What about the proximal stent deformation after POT and drawing out the SB jailed wire, caused by GC deep engaging? It's better to draw out the SB wire before POT?
Very clear images in cartoons and videos.thanks
Re POT is mandatory in all bifurcation stenting techniques
I finde it very effective , useful and tutorial thanks