11 Feb 2022
Cusp overlay implantation technique – planning step-by-step
The cusp-overlay method aims to implant the self-expandable device higher than in former ways without device pop-out upon release and it reduces pacemaker rates significantly.
Frequency of the problem:
Expert level:
Summary
Unlike balloon-expandable valves which require a coplanar projection with 3 cusps, additional steps are taken when implanting a self-expandable valve, for example, Corevalve/Evolut-R/Pro-Platforms. A coplanar projection by overlapping the right coronary cusp (RCC) and left coronary cusp (LCC) offers several potential advantages.
Finally, the cusp-overlay method aims to implant the self-expandable device higher than in former ways without device « pop-out upon release and it reduces pacemaker rates significantly.
In cusp-overlay view you can:
- eliminate the parallax of the delivery catheter
- observe the deployment in true coplanar view
- work with a shorter visual distance for Corevalve/Evolut-Platforms to engage the non-coronary cusp (NCC) and LCC
The problem
Various methods have been suggested for determination of the optimal projection for transcatheter aortic valve replacement (TAVR). Balloon-expandable transcatheter heart valves (THVs) are commonly centred and deployed in a perpendicular view of the aortic valve annulus, with the RCC projected between NCC and LCC.
Self-expanding THVs, however, engage the aortic valve from the outer aortic curvature and are deployed from the NCC toward the LCC.
Even with new generation self-expandable THV-Devices such as Corevalve/Evolut-Platforms, the occurrence of conduction disturbances requiring pacemaker implantation is a significant concern. In contrast to classical implant-views (3 cusps), cusp-overlay technique promises the visualization of the real implantation depth.
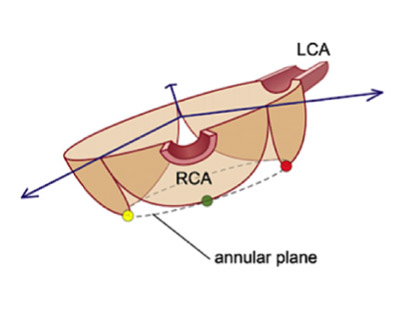
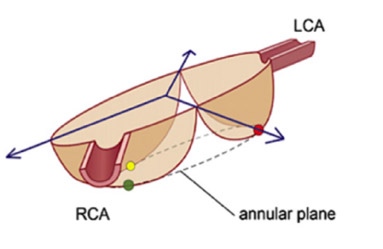
Principal idea
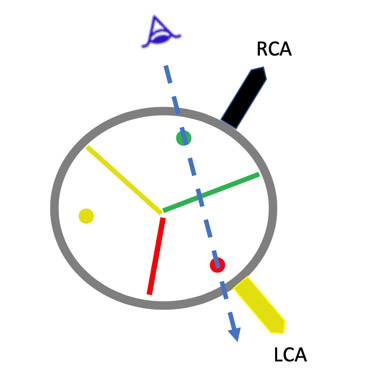
The cusp-overlay method aims to define optimal fluoroscopic projections for TAVR with a self-expandable device. Optimal projection is generated by overlapping the RCC to the LCC. The non-right commissure is displayed in the centre of the fluoroscopic image, allowing the interventionalists to deploy the device relative to the membraneous septum and hence the conduction system below the atrioventricular node.
Almost always cusp overlay view results in right anterior oblique (RAO) and caudal (CAU). The view isolates the NCC to provide accurate assessment of deployment depth and elongates the view of the left ventricular outflow tract (LVOT).
At the level of NCC, the correct implantation plane for deployment of TAVI achieves higher implants with more control and lower pacemaker rates by less interaction with conduction system. The NCC nadir is better visualized, allowing higher valve deployment with a lower risk of « pop-out ».
In patients with challenging body habitus such as obesity, an RAO, caudal view may reduce fluoroscopic image quality, and certain extreme RAO, caudal angles may not be possible to create the cusp-overlap view.
In those instances, we perform e.g. Evolut - TAVI using a 3-cusp view or overlapping the NCC and the RCC in an LAO cranial view. Contemporary implant techniques of modern self-expandable TAVI-platforms (e.g. Evolut/Acurate/Navitor) using cusp-overlay technique also for commissural alignment aspects for coronary artery cannulation after TAVI.
Material needed
Planning of the mentioned cusp-overlay technique is possible with dedicated software tools like 3mensio valves software (Pie Medical Imaging; Maastricht, the Netherlands) using multi-detector computed tomography (MDCT) data set.
Method step-by-step
Step 1 - Preprocedural Evaluation and assessment of MDCT Scan
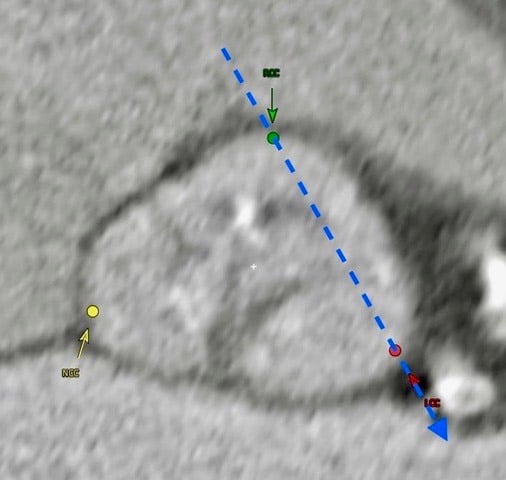
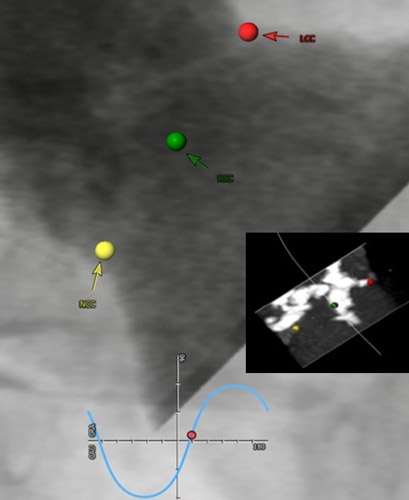
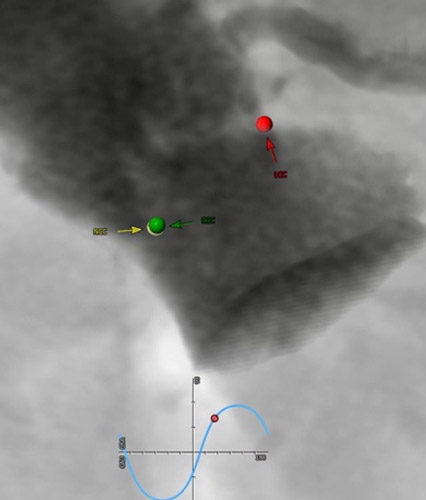
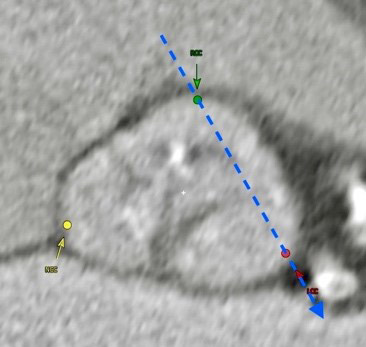
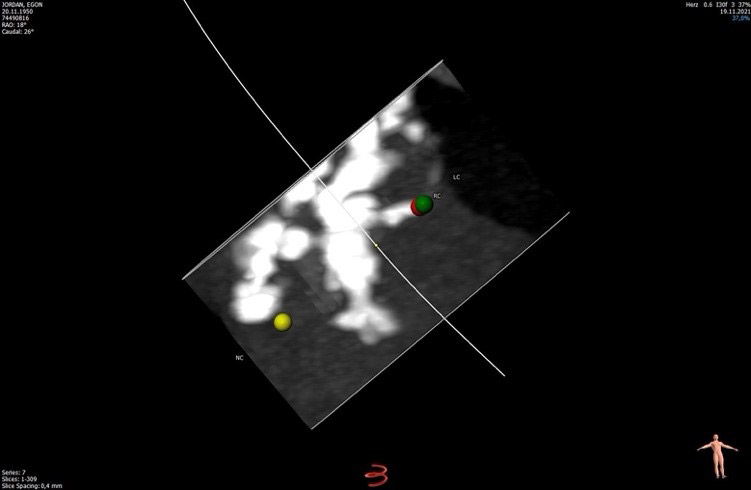
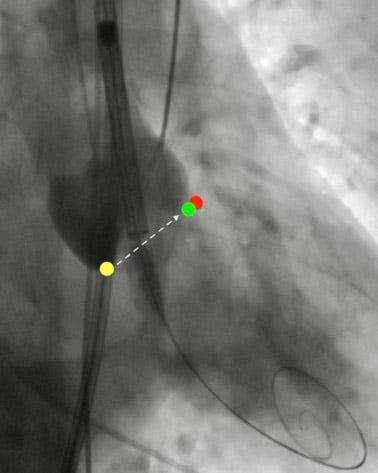
RCC/LCC cusp overlay view - RAO 12 CAUD 20
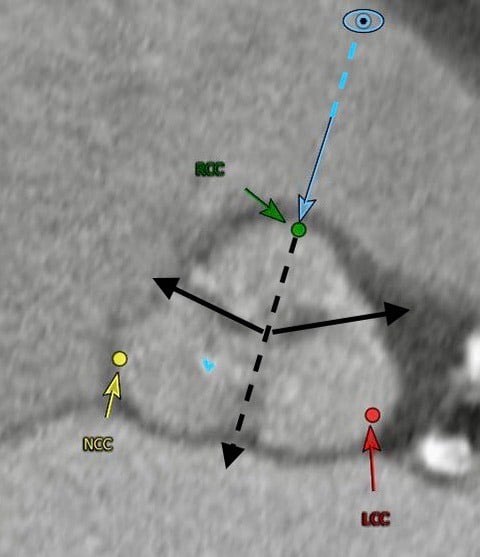
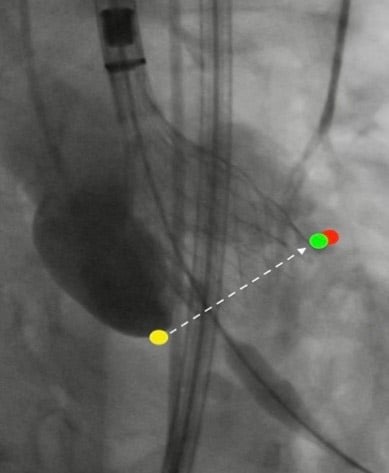
Three cusp coplanar view - LAO 27 CRAN 5
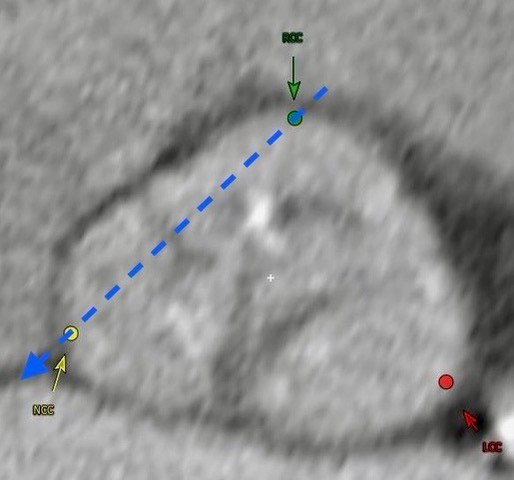
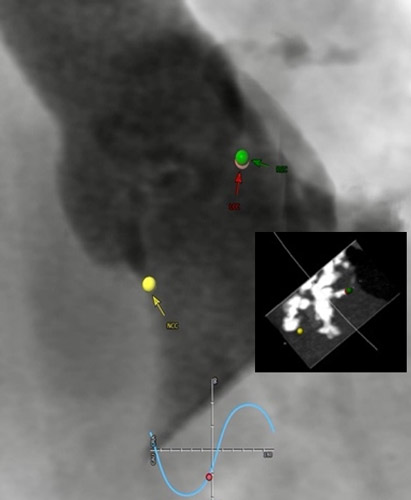
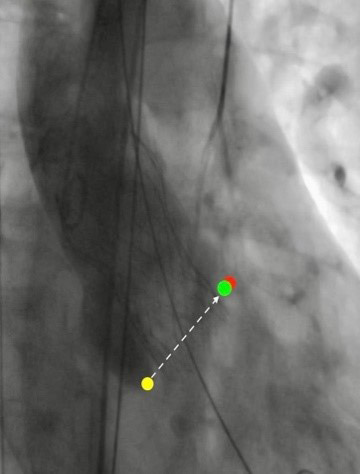
RCC/NCC cusp overlay view - LAO 31 CRAN 23

Credit: Bielauskas et al. JACC 2021
Credit: Bielauskas et al. JACC 2021
Credit: Bielauskas et al. JACC 2021
RAO 12 CAUD 20
LAO 27 CRAN 5
LAO 31 CRAN 23
Step 2 - Implantation technique in RCC/LCC cusp overlay technique
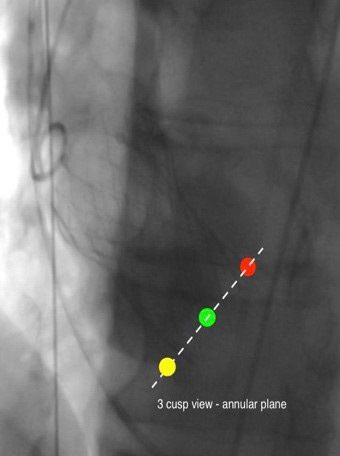
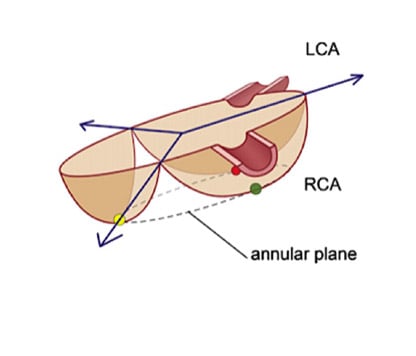
3 cusp view - annular plane
Points of specific attention
- obligatory is a cross-check in 3cusp (true coplanar) view for implantation depth in LCC area before final release
- in 3 cusp-view, eliminate the parallax of the delivery catheter
- keep the calcium burden and its distribution (known from the MDCT reconstruction) in every TAVI – step in mind
- assessment of aortic delivery catheter positioning in LAO
A word from the reviewer - Alexander Wolf
The cusp overlay technique is helpful not only in achieving a higher implant with the Corevalve Evolut platform - and therefore it can help to reduce pacemaker rate post-TAVI, but it also plays a role in commissural alignment with various self-expandable transcatheter aortic valve systems.




3 comments
Great message and analysis.
Very useful and practical
EXCELLENT TECHNIQUE PROF.G.S.N.M.RAO MD.,DM