13 Sep 2023
Commissural alignment during TAVI
A problem-solving step by step tutorial
As lifetime management of aortic valve disease patients undergoing TAVI is gaining increased attention, this article sought to summarize the principal idea and possible technical implementation of commissural alignment with current generation transcatheter heart valves (THVs).
Frequency of the problem:
Expert level:
Summary
The anatomy of the aortic root complex helps maintain a laminar blood flow to the peripheral vessels, mainly during systole, as well as sinus & coronary perfusion during diastole. Aortic valve interventions are therefore currently evolving from merely treating the diseased aortic valve to preserving the aortic root complex anatomy.
Commissural alignment is defined as the angular relationship between native and bioprosthetic commissures after biological valve implantation (surgical or transcatheter). While commissural alignment is almost always performed during surgical aortic valve replacement, its importance and implementation during transcatheter aortic valve implantation (TAVI) has only been recently recognized. Proper alignment has been shown to affect coronary access post-TAVI, may positively contribute to coronary filling, valve hemodynamics and leaflet stress, and may also facilitate redo-procedures.
As lifetime management of aortic valve disease patients undergoing TAVI is gaining increased attention, we sought to summarize the principal idea and possible technical implementation of commissural alignment with current generation transcatheter heart valves (THVs).
The problem
The degree of commissural misalignment, corresponding to the risk of overlap between the neo-commissures and the native coronary ostia, should be ideally kept to a minimum. Unlike surgeons, who have an unrestricted view of the native aortic valve and its commissures during surgery, interventional cardiologists have to deduce the position of the native commissures from 2-dimensional angiographic images, and orientate THVs of different design (supra- vs intra-annular leaflet position, closed vs open cell design), some of which lack neo-commissural angiographic markers, in order to achieve commissural alignment.
Severe misalignment has been shown to hinder coronary access post-TAVI in clinical studies, especially with long-stent frames and supra-annular leaflet design1,2. In the context of a redo-TAVI, a significant coronary-commissure overlap would yield leaflet modification futile.
Principal idea
Achieving a successful commissural alignment, defined as ≤ 30° deviation between native and neo-commissures1, is both patient- as well as THV-dependent. Demarcation of the native commissures is achieved by rotating the C-arm to a pre-procedurally identified non-coronary cusp (NCC) / right coronary cusp (RCC) and NCC / left coronary cusp (LCC) commissural overlap view, isolating therefore the inter-coronary commissure to the right side of the screen3,4.
Ideally, the THV neo-commissures should then be fluoroscopically marked and rotated by the implanter, so that one neo-commissure overlaps with the isolated inter-coronary commissure before implantation.
Material needed
1 - Identification of the native commissures
The fluoroscopic projections that mark the positions of the native commissures are identified from the pre-TAVI computed tomography (CT), which are then used to angulate the C-arm for orientation during implantation:
- 3-cusp co-planar view: the 3 commissures are in an anticipated I-I-I configuration.
- Cusp-overlap view: isolating the intercoronary commissure (LCC-RCC) on the right side of the image, and the whole NCC on the left side3-5 (Figure 1).
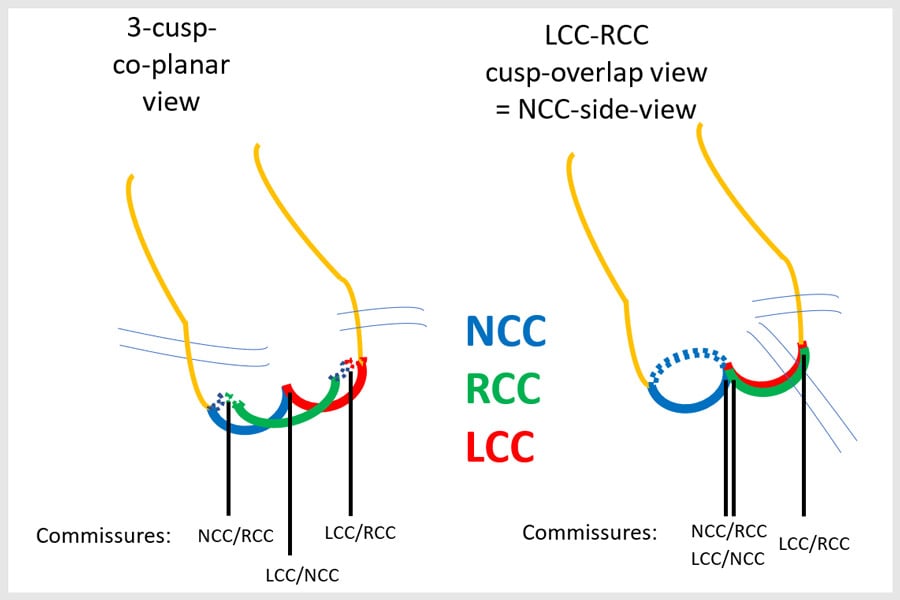
Figure 1: Commissural position in 2 fluoroscopic views required to achieve commissural alignment; the 3-cusp-coplanar view and the LCC-RCC cusp-overlap view.
2 - Identification of the THV commissures
This depends on the design of the THV and the presence of fluoroscopic markers for the neo-commissural posts that can be identified during implantation.
With current THVs, the following possibilities are available:
1. Directly identifiable neo-commissural posts: the commissural posts are easy to identify, and their unique design allows fluoroscopic recognition of their angulation and orientation according to native anatomy.
A typical example is the Acurate neo/neo2 platform (Boston Scientific) (Figures 2-4).
The commissural posts of the Portico/Navitor THV (Abbott) can similarly be identified on fluoroscopy, but these are not particularly radiopaque and less clearly visible compared to the Acurate neo/neo2 THV6.
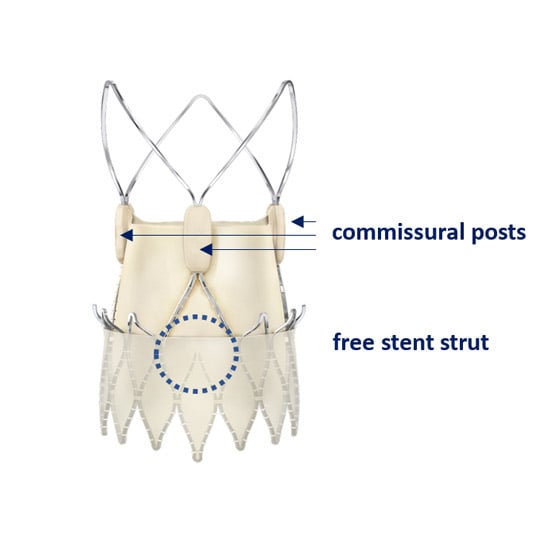
Figure 2: Commissural posts of the Acurate neo2 valve. Note that each post also corresponds to a free stent strut located below the commisure
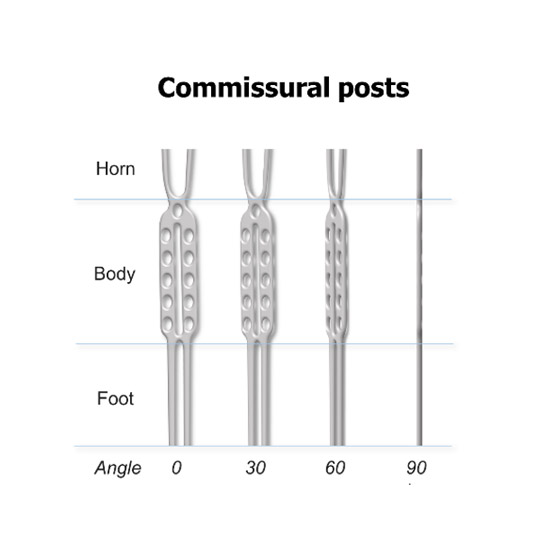
Figure 3: Fluoroscopic appearance of the Acurate neo2 commissural posts from different angulations. Reproduced with permission from ref. 4
Figure 4: Optimal orientation of the neo-commissural posts of the Acurate neo/neo2 platform before (left panel) and after (right panel) valve implantation
2. Commissures are not directly identified, but indirect markers for the commissures exist on the catheter or delivery system.
A typical example for that is the Evolut R/Pro/Pro+ platform (Medtronic). The Evolut THV lacks direct visual markers for its neocommissures, but the “C-paddle”, which extends from the THV outflow and is angiographically visible after full release of the THV, corresponds to a neocommissure6,7. This C-paddle is always mounted 90° clockwise from the so-called fluoroscopic “Hat” marker, which is a visible marker on the delivery catheter while the THV is being tracked and positioned7. Thus, if the “Hat” marker can be oriented to the center front in the cusp-overlap view during valve implantation, the C-paddle, with its corresponding commissure, would align itself with the isolated inter-coronary commissure3 (Figures 5-8).
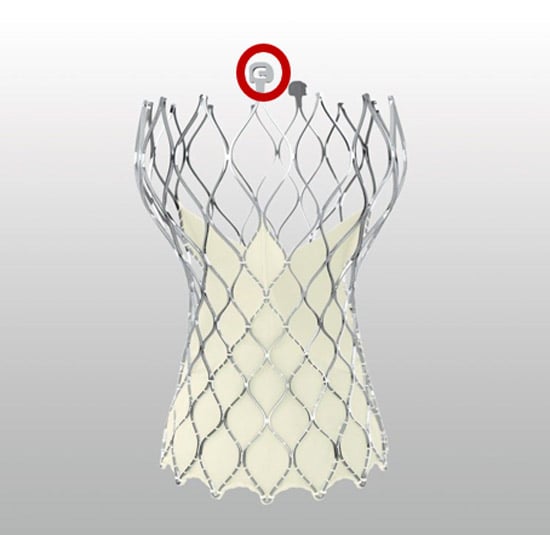
Figure 5: The C-paddle of the Evolut platform (red circle) always corresponds to one of the three commissures
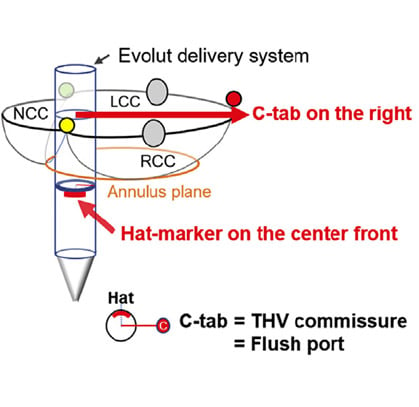
Figure 6: Schematic demonstrating the spatial relationship between the C-paddle of the Evolut stent and the “Hat” marker on the delivery catheter. Reproduced with permission from ref. 3.
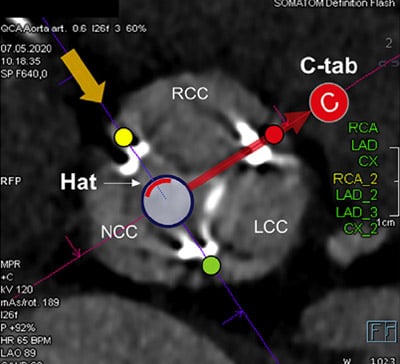
Figure 7: Spatial relationship between the C-paddle of the Evolut stent and the “Hat” marker on the delivery catheter in a short axis computed tomography image. Reproduced with permission from ref. 3.
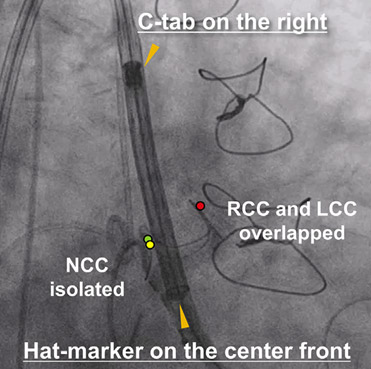
Figure 8: Spatial relationship between the C-paddle of the Evolut stent and the “Hat” marker on the delivery catheter in the cusp-overlap view. Reproduced with permission from ref. 3.
Importantly, while the commissural posts of balloon-expandable THVs can be identified on fluoroscopy after valve implantation, this is not the case when the THV is still crimped. Furthermore, there is no method to facilitate commissural alignment with current-generation balloon-expandable THVs through a specific valve orientation during initial crimping6.
Therefore, commissural alignment cannot be currently standardized with balloon-expandable THVs, and will not be described in the following step-by-step approach. This may change with next generation devices.
Method step-by-step
Step 1: Introducing the delivery system (passive alignment)
- Due to the alignment of flush port and a neocommissure, introduction of the delivery system with the flush port rotated to 6 o’clock position (pointing downwards) achieves commissural alignment in more than 80 % of cases with the Acurate neo/neo2 platform8 (Figure 9).
- Introduction of the delivery system with the flush-port rotated to the 3 o’clock position (looking towards patient’s left side) achieves a hat-marker orientation that achieves commissural alignment in more than 70 % of the cases with the Evolut platform7 (Figure 10).
- Because the attachment of the Portico/Navitor THV to its delivery system is not consistent, no recommendation can be currently made for a specific orientation of the delivery catheter during the advancement of this THV6.

Figure 9: Introduction of the Acurate neo2 platform with the flushport at 6 o’clock. Reproduced with permission from ref. 8


Figure 10: Introduction of the Evolut platform with the flushport at 3 o’clock
Step 2: Valve position in the 3-cusp co-planar view
- Acurate neo2 and Portico/Navitor platforms: I-I-I configuration of the commissural posts with one non-angled post at “centre back” and two 60° angled posts at both sides (Figure 11). Visualization is less clear with the Protico/Navitor valve. As the posterior location of the central post is difficult to ascertain in this view, this configuration corresponds to either correct alignment (if the central post is posterior) or complete misalignment (if the central post is anterior). A clearer differentiation can be done in the cusp-overlap view.
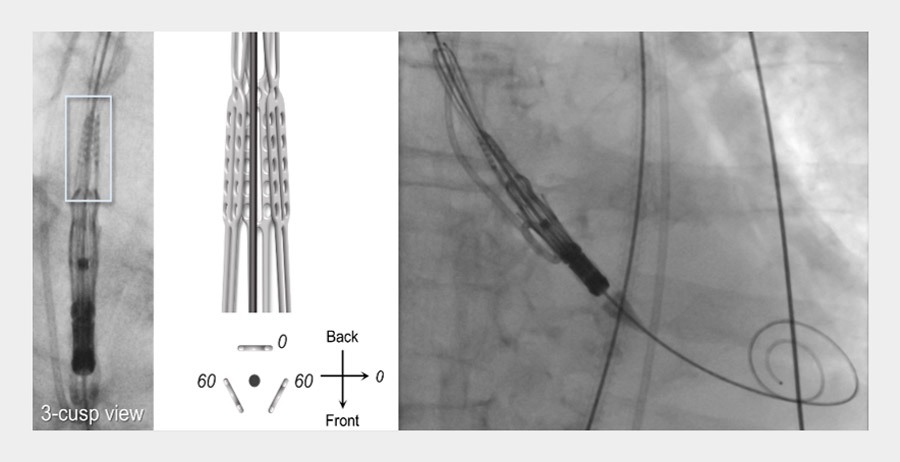
Figure 11: I-I-I fluoroscopic appearance of the 3 commissural posts of the Acurate neo2 valve in the 3-cusp view with the central post located posteriorly, corresponding to correct alignment.
- Evolut platform: “Hat” marker orientation to the outer curve of the aorta on the left side of fluoroscopic image (Figure 12).

Figure 12: Two examples of an Evolut THV with the “Hat” marker oriented towards the outer curve of the aorta
Step 3: Valve position in the L / R cusp-overlap view
- Acurate neo2 and Portico/Navitor platforms: II-I-configuration of the commissural posts isolating the dedicated “intercoronary” THV commissure on the right side of the image (in a 90° angle) overlapping the anticipated intercoronary commissure of the native valve (Figure 13).
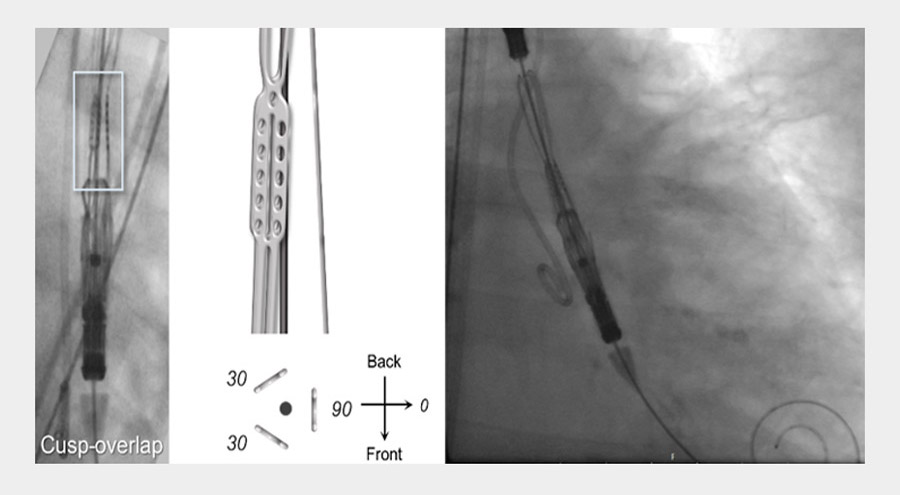
Figure 13: II-I fluoroscopic appearance of the 3 commissural posts of the Acurate neo2 valve in the cusp-overlap view, corresponding to correct alignment.
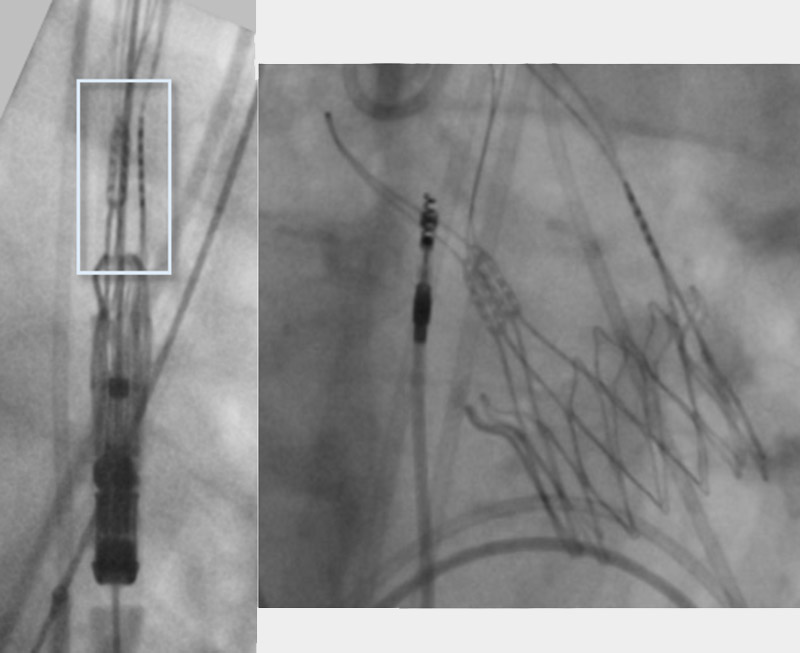
- Evolut platform: C-Paddle as A surrogate marker for the “intercoronary” THV commissure on the right side of the image, which should co-localize in a 90° angle to the hat marker of the delivery system on the center front (Figure 14)
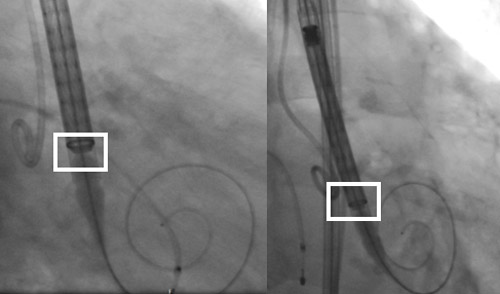
Figure 14: Two examples of an Evolut THV with the “Hat” marker (white box) oriented towards the center front in the cusp-overlap view, indicating commissural alignment.
Step 4: Active optimization
If the valve position does not indicate optimal commissural alignment as indicated in Step 3, turning the delivery catheter can actively change commissural orientation, and match the neo-commissures to the native ones, as desired. However, this requires a flexible delivery catheter that allows some degree of rotation without resistance or excessive torque. This active optimization of commissural alignment can be obtained with the Acurate neo2 platform, as well as the Portico/Navitor system (if posts can be fluoroscopically identified as previously mentioned).
The Evolut system is significantly less flexible, and although it can be rotated, there is no standardized method for delivery catheter manipulation with the currently available platforms (R/Pro/Pro+) that we feel we can safely recommend. The newer generation Evolut Fx system is more flexible and can probably be easily adjusted, but it is not yet available in Europe.
Active optimization of the Acurate neo2 valve is summarized below (Figures 15-18). For easier identification of fluoroscopic orientation, assessment can be done in the 3-cup view and rotation in the cusp-overlap view.

Figure 15: II-I configuration of the Acurate neo2 valve on 3-cusp coplanar view (images from micro-CT and fluoroscopy). This configuration implies the need for a clockwise rotation of the delivery catheter to obtain commissural alignment. Micro CT images used with permission from Boston Scientific
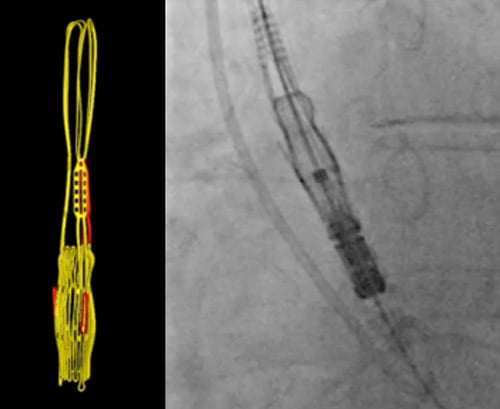
Figure 16: I-II configuration of the Acurate neo2 valve on 3-cusp coplanar view (images from micro-CT and fluoroscopy). This configuration implies the need for a counter-clockwise rotation of the delivery catheter to obtain commissural alignment. Micro CT images used with permission from Boston Scientific
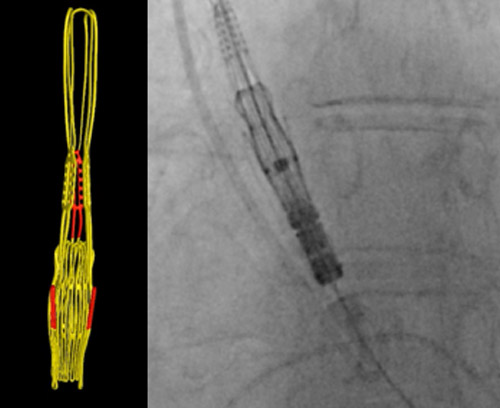
Figure 17: Correct (I-I-I) configuration of the Acurate neo2 valve on 3-cusp coplanar view with the central post located posteriorly (images from micro-CT and fluoroscopy). Micro CT images used with permission from Boston Scientific
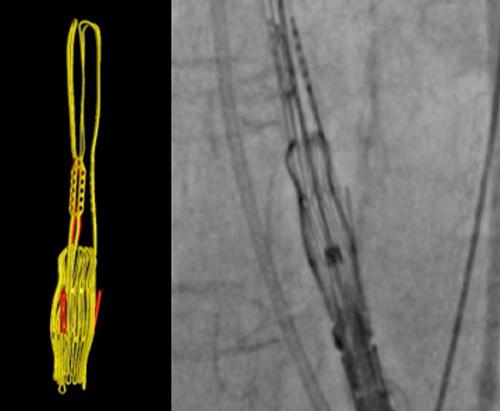
Figure 18: Correct (II-I) configuration of the Acurate neo2 valve on cusp-overlap view (images from micro-CT and fluoroscopy). Micro CT images used with permission from Boston Scientific
Step 5: Valve deployment
Valve deployment should then be performed according to the specific valve platform.
Commissural alignment can be fluoroscopically assessed after final device deployment in both in the 3-cusp-view and in the cusp-overlap-view:
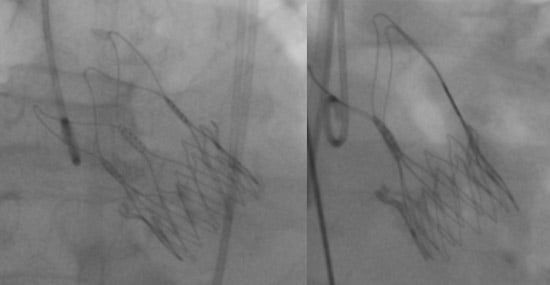
Figure 19: Correct configuration of the Acurate neo2 valve after implantation on 3-cusp view (I-I-I configuration, left panel) and cusp-overlap view (II-I configuration, right panel)
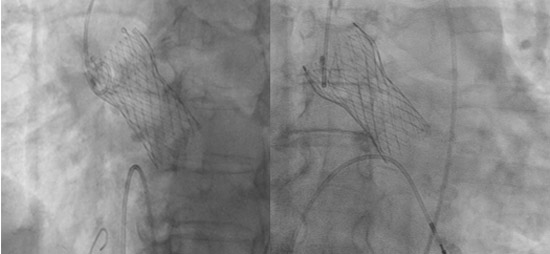
Figure 20: Correct configuration of the Evolut valve after implantation on 3-cusp view (C-Paddle oriented towards the inner aortic curve, left panel) and cusp-overlap view (C-Paddle on the right side, right panel).
Points of specific attention
Handle turns are not linear for valve rotation
- 0 - 0.5 turn = very little valve rotation
- 0.5 - 1 turn = typical desired valve rotation
- 1-1.5 turns = valve rotation may be excessive
A word from the reviewer

This article of the TAVI team at the Heart Center Leipzig is a state of the art description of commissural alignment with current THV devices. Very important, since our daily practice treats more lower risk and younger patients, raising the issue of providing coronary re-access.
References
- Fuchs A, Kofoed KF, Yoon SH, Schaffner Y, Bieliauskas G, Thyregod HG, Makkar R, Søndergaard L, De Backer O, Bapat V. Commissural alignment of bioprosthetic aortic valve and native aortic valve following surgical and transcatheter aortic valve replacement and its impact on valvular function and coronary filling. JACC Cardiovasc Interv 2018;11:1733-1743.
- Tarantini G, Nai Fovino L, Scotti A, Massussi M, Cardaioli F, Rodinò G, Benedetti A, Boiago M, Matsuda Y, Continisio S, Montonati C, Cacciavillani L, Pavei A, Masiero G, Napodano M, Fraccaro C, Fabris T, Iliceto S. Coronary access after transcatheter aortic valve replacement with commissural alignment: the ALIGN-ACCESS study. Circ Cardiovasc Interv 2022;15:e011045.
- Kitamura M, Wilde J, Dumpies O, Gutberlet M, Gohmann R, Shibata M, Noack T, Thiele H, Holzhey D, Abdel-Wahab M. Patient-Specific Neocommissural Alignment of the Evolut Valve: A Pilot Study in Transcatheter Aortic Valve-in-Valve Replacement. JACC Cardiovasc Interv 2021;14:934-936.
- Kitamura M, Wilde J, Gohmann R, Majunke N, Gutberlet M, Shibata M, Kiefer P, Desch S, Thiele H, Holzhey D, Abdel-Wahab M. Commissural Alignment of the ACURATE neo Valve in Transcatheter Aortic Valve Replacement. JACC Cardiovasc Interv 2021;14:1740-1742.
- Ben-Shoshan J, Alosaimi H, Lauzier PT, Pighi M, Talmor-Barkan Y, Overtchouk P, Martucci G, Spaziano M, Finkelstein A, Gada H, Piazza N. Double S-Curve Versus Cusp-Overlap Technique: Defining the Optimal Fluoroscopic Projection for TAVR With a Self-Expanding Device. JACC Cardiovasc Intervention 2021;14:185-194.
- Tang GHL, Amat-Santos IJ, De Backer O, Avvedimento M, Redondo A, Barbanti M, Costa G, Tchétché D, Eltchaninoff H, Kim WK, Zaid S, Tarantini G, Søndergaard L. Rationale, definitions, techniques, and outcomes of commissural alignment in TAVR: from the ALIGN-TAVR consortium. JACC Cardiovascular Interventions 2022;15:1497-1518.
- Tang GHL, Zaid S, Fuchs A, Yamabe T, Yazdchi F, Gupta E, Ahmad H, Kofoed KF, Goldberg JB, Undemir C, Kaple RK, Shah PB, Kaneko T, Lansman SL, Khera S, Kovacic JC, Dangas GD, Lerakis S, Sharma SK, Kini A, Adams DH, Khalique OK, Hahn RT, Søndergaard L, George I, Kodali SK, De Backer O, Leon MB, Bapat VN. Alignment of Transcatheter Aortic-Valve Neo-Commissures (ALIGN TAVR): Impact on Final Valve Orientation and Coronary Artery Overlap. JACC Cardiovasc Interv. 2020;13:1030-1042.
- Abdel-Wahab M, Kitamura M, Fitzgerald SJ, Dumpies O, Wilde J, Gohmann RF, Majunke N, Gutberlet M, Kiefer P, Noack T, Lurz P, Desch S, Frawley C, Ward K, Borger MA, Holzhey D, Thiele H. Neo-Commissural Alignment Technique for Transcatheter Aortic Valve Replacement Using the ACURATE Neo Valve. Circ Cardiovasc Interv 2022;15:e011993.
Authors





4 comments
Great lesson, easy but important. Thanks a lot Dr. Abdelahafez et als.
very nice illustration thanks alot
Very informative,practical and to the point tips, good effort, chapeau all guys
Very informative,practical and to the point tips, good effort, chapeau all guys