How to retrieve your Prostyle when it gets stuck
A problem-solving step by step tutorial
In challenging anatomies, the Prostyle may get stuck due to calcification, leading to urgent vascular surgery and increasing the operative risk for the patients. This tutorial shows a step-by-step bailout procedure to mitigate risks and ensure patient safety.
Frequency of the problem:
Expert level:
Summary
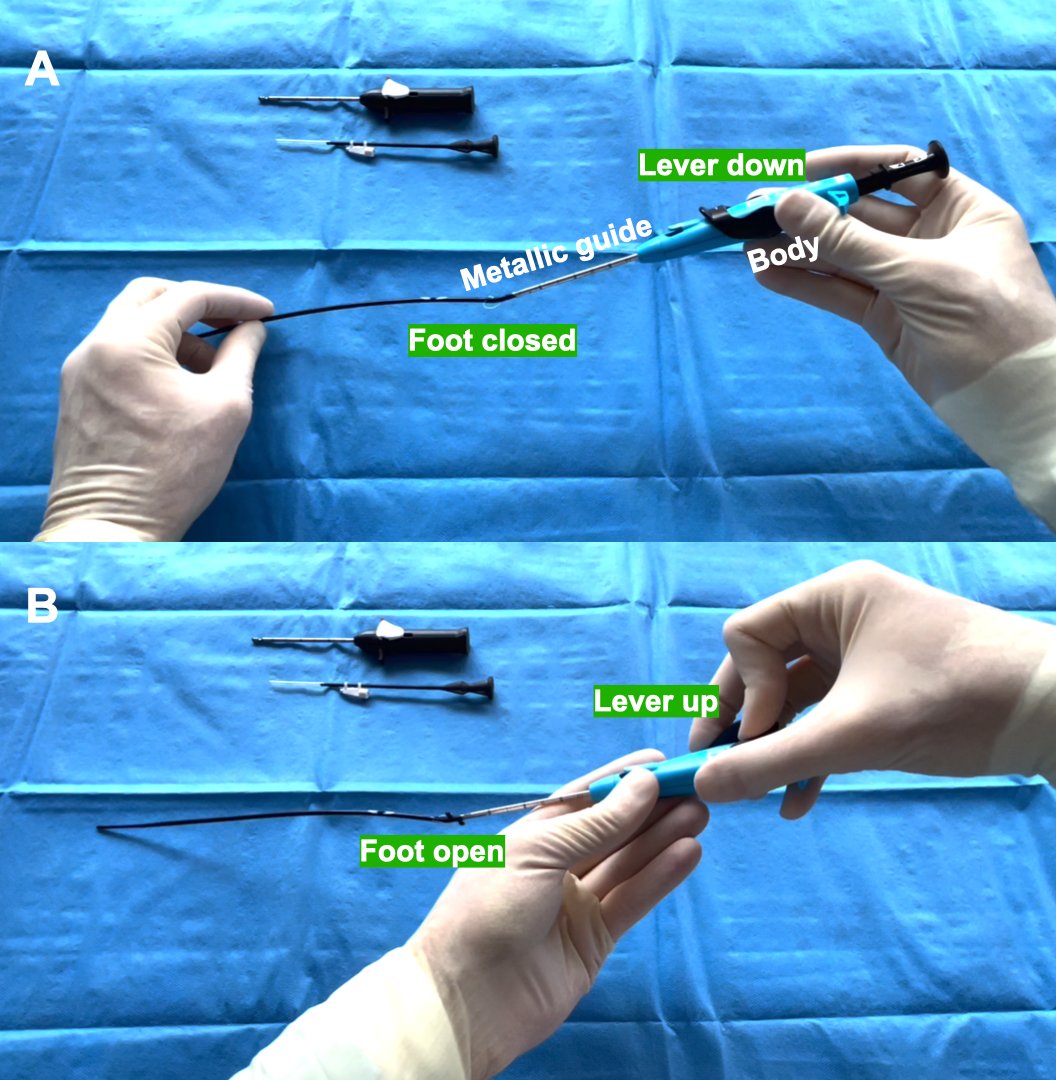
The Perclose Prostyle is a suture-mediated closure system (Figure 1A). It has been approved to close large bore accesses, making it widely used in CathLabs due to the rapid development of structural interventional cardiology.
A guidewire is necessary to insert the device. When blood spills, the guidewire is withdrawn. Then, a lever allows to open the device “foot” and the pullback provides contact with the arterial wall (Figure 1B). Hence, a needle is deployed and the suture loop is formed.
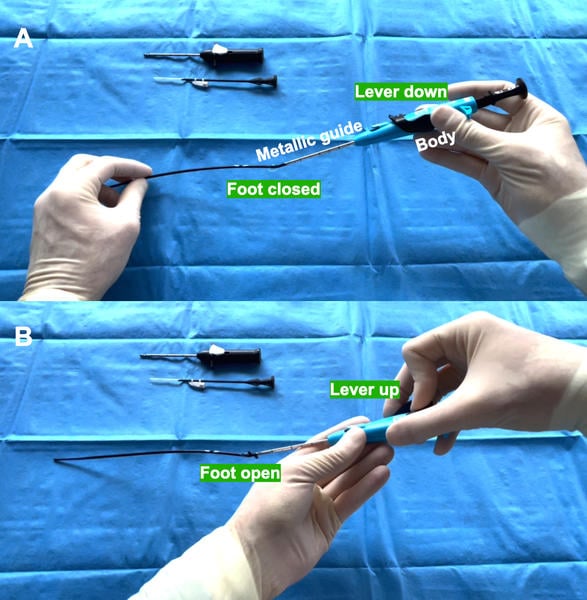
Figure 1:
A) Main components of the Prostyle device.
B) Illustration demonstrating the raising of the lever resulting in foot opening.
The Problem
In calcific and complex anatomies, it could happen that the Prostyle gets stuck. Indeed, it is necessary to close the foot through the lever in order to retrieve the device.
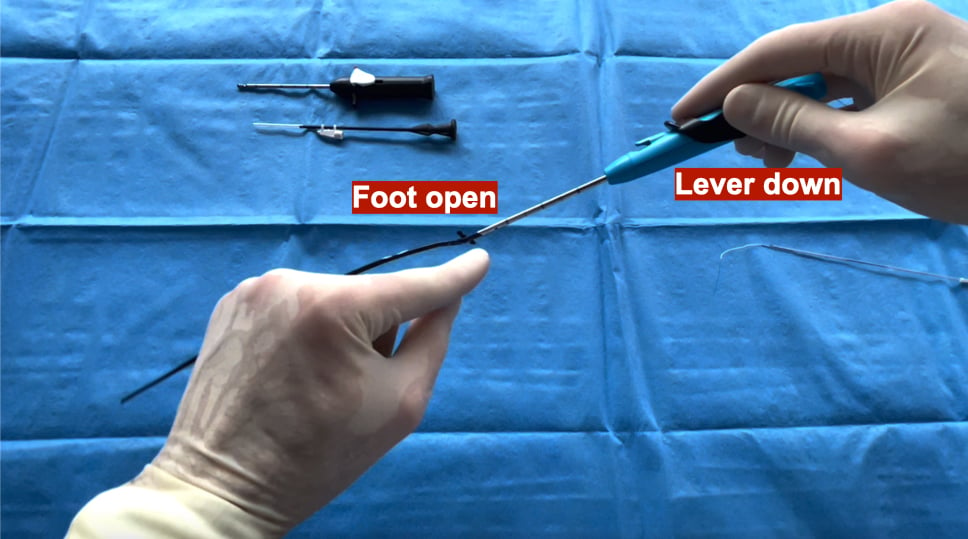
However, the high burden of calcium can block the foot in the arterial wall and when the lever is lowered, the foot remains open, due to an uncoupling of the system (Figure 2).
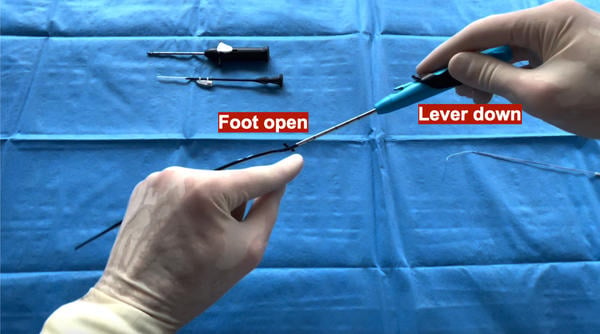
Figure 2: Uncoupling of the foot from the lever in the Prostyle device, leading to device entrapment in calcific and complex anatomies.
In these cases, urgent vascular surgery is required, increasing the operative risk for the patients.
Principal idea
The main idea is to “recouple” the system to avoid the necessity of an invasive procedure such as open surgery to withdraw the device. In fact, patients treated with the Prostyle are often frail, especially the ones undergoing TAVI and a rapid bailout technique can change the outcomes.
Material needed
The material needed consists of a stuck and uncoupled Prostyle.
Method step-by-step
Step 1
After having verified the impossibility of extracting the device with the traditional manoeuvres, it is necessary to grab the metallic guide of the Prostyle device with the left hand and its body with the right hand. (Figure 3A).
Step 2
The left hand must hold still and the right hand has to perform a combination of translational and rotational movements of the Prostyle body (Figure 3B) until the metallic guide is broken at its proximal part (Figure 3C).
Step 3
The right hand must keep the lever down and the Prostyle body has to be pushed towards the left hand to close the device foot (Figure 3D). Thus, the device can be safely retired (Video 1).

Figure 3: Step-by-step bailout procedure for a stuck Prostyle device due to uncoupling.
A) Initial grabbing of the metallic guide and body.
B) Translational and rotational movements to break the metallic guide.
C) Metallic guide broken at its proximal part.
D) Closure of the device foot by pushing the body towards the left hand while keeping the lever down.

Points of specific attention
- During the whole manoeuvre, the left hand has to perform a gentle push to disengage the foot at least partially from the vessel. Then, it has to avoid any other movement to prevent vessel damage: only the right hand accomplishes all the work.
- Usually, this procedure does not affect the suture deployment, however a guidewire can be put in place to secure the access.
A word from the reviewer - Radoslaw Parma

Percutaneous vascular closure troubleshooting skills are precious and hard to find. They prevent high-risk complications in vulnerable patients treated with large-bore vascular access.
The Toulouse team presents a unique solution to tackle a trapped Prostyle device during removal. This sporadic problem is mostly encountered in patients with highly calcified arterial walls or steep vascular access angulation. A stuck device footplate disconnects from the handle lever, leading to problems in retrieving the device from the punctured artery.
The ingenious recommendation allows operators to push the footplate back to its coaxial position and remove the Prostyle system. It saves the operators from tedious attempts to split the blue handle open, the process hindered by the surrounding black lever, to gain access to the internal locking mechanism. I am grateful to the authors for publishing their experiences to help their colleagues and patients in need.
Attitudes:
- The skill should be shared among advanced operators, who can balance the risk of medical device disassembly in high vascular risk scenarios
- Failed attempts to retrieve the device should lead to urgent and safest surgical access site treatment
- Collagen-based vascular closure know-how complements suture-based device expertise. The two techniques may be combined for rescue situations.
Additional skills:
- Ultrasound imaging can detect the footplate and metal guide position in the artery and assess the arterial access site after the device is removed and the vessel is closed.
- Fluoroscopy with digital subtraction angiography at appropriate C-arm angulations may help recognise the footplate position inside the arterial lumen and the presence of arterial dissection or bleeding.
- Wire introduction before Prostyle removal provides options to complete arterial closure with a collagen-based occluder if a Prostyle suture fails to seal the access site completely.
Authors




No comments yet!