01 Jun 2026
A novel bailout technique for the percutaneous extraction of an entrapped coronary guidewire beneath a crushed stent
A problem-solving step-by-step tutorial
A simple bailout technique for guidewire entrapment beneath a crushed stent, enabling safe and controlled extraction.
Frequency of the problem:
Expert level:
Summary: external stabilisation technique for guidewire extraction
Guidewire entrapment beneath a crushed stent is a rare but potentially catastrophic complication during PCI, often resistant to conventional retrieval strategies.
We describe a simple and reproducible bailout technique based on external mechanical stabilisation of the guidewire using a needle holder applied at the distal guidewire end.
By firmly grasping both the inner core and outer coil of the wire, this method prevents elastic elongation and allows effective transmission of traction forces.
Under continuous fluoroscopic guidance, controlled, coaxial traction enables safe disengagement of the wire without fracture or vessel injury.
This technique requires no additional intravascular equipment and can be rapidly implemented when standard approaches fail or become unsafe. It represents a practical solution grounded in wire mechanics and may help operators avoid surgical bailout in complex PCI scenarios.
The problem: limitations of conventional retrieval techniques
Guidewire entrapment, particularly beneath a crushed stent, may render conventional retrieval techniques ineffective.
Standard methods (small balloon, snare, microcatheter, guide-extension catheter) can fail due to inability to transmit sufficient traction force or risk of wire fracture and vessel injury.
A key limitation is the tendency of the guidewire inner core to elongate under traction, dissipating force and preventing effective extraction. In such cases, operators face limited options, including high-risk aggressive traction or emergency surgery.
Principal idea: mechanical stabilisation for guidewire extraction
The technique consists of externally clamping the guidewire with a needle holder at the sheath entry site to lock together the outer coil and inner core. This prevents differential elongation and enables uniform force transmission along the wire.
Controlled, coaxial traction is then applied under fluoroscopy, allowing progressive disengagement of the entrapped segment.
The key concept is mechanical stabilisation of the wire structure to overcome elastic recoil and restore effective traction dynamics.
Material needed
- Standard coronary guidewire (entrapped)
- Radial or femoral vascular access sheath and standard PCI setup
- Needle holder (Kocher-type forceps)
- Fluoroscopy imaging
Step-by-step method
Step 1: guidewire entrapment
(Figure 1) – Confirm entrapment and failure of standard techniques
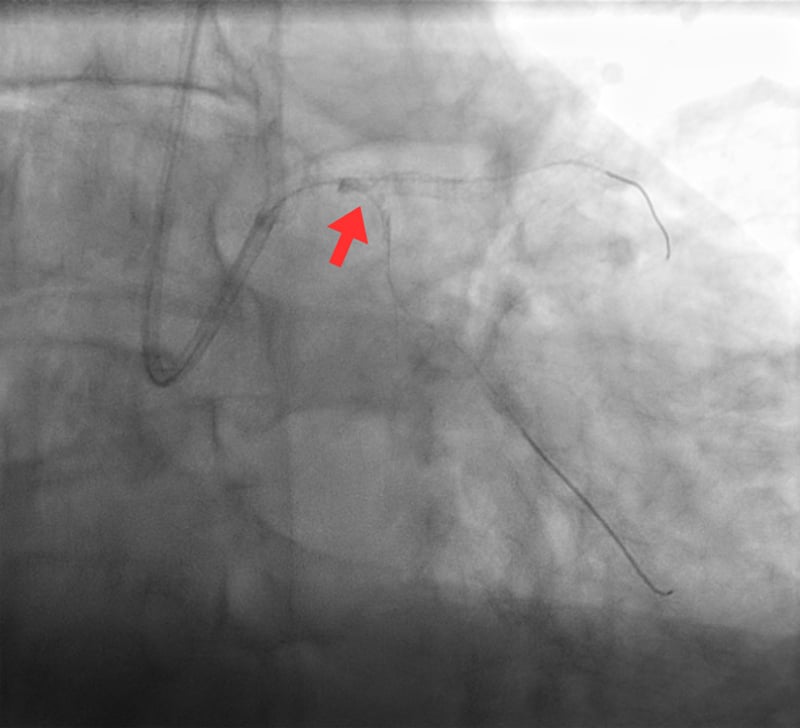
Figure 1. Guidewire entrapment - Fluoroscopic image demonstrating the obtuse marginal guidewire firmly jailed and entrapped beneath the crushed stent at the level of the left main–left circumflex bifurcation (arrow).
- Verify fluoroscopically that the guidewire is jailed beneath stent struts
- Try as a first attempt: gentle, smooth, and strictly coaxial manual traction
- If unsuccessful, proceed stepwise with conventional retrieval techniques:
- Small-balloon technique (inflate and withdraw)
- Microcatheter or trapping-balloon-assisted retrieval
- Snare retrieval (if an accessible segment is available)
- Guide-extension catheter to improve support and coaxiality
- Discontinue these approaches if ineffective or if increasing resistance, wire deformation, or risk of vessel injury is observed
Step 2: prepare external access to the wire
- Maintain guidewire position (do not cut or withdraw partially)
- Expose the distal segment of the wire at the Y-connector entry hub
- Ensure stable guide catheter position and coaxial alignment
Step 3: external stabilisation of the guidewire
(Figure 2 A-B) – Secure the wire and lock mechanical integrity

Figure 2 A-B. External stabilization of the guidewire - A needle holder (Kocher-type forceps) is applied to the distal external segment of the guidewire (5–10 cm from the Y-connector), firmly locking both inner core and outer coil to prevent slippage and allow effective traction.
- Apply the needle holder firmly to the distal external segment of the guidewire (approximately 5–10 cm from the Y-connector entry site)
- Lock the needle holder to achieve a tight grip and ensure simultaneous capture of both the inner core and outer coil
- Confirm absence of slippage to prevent independent movement of core and coil before traction
- Hold the needle holder with the right hand while stabilizing the Y-connector and guiding catheter with the left hand to prevent inadvertent disengagement or loss of coaxial alignment
- Ensure the guiding catheter remains stable and well engaged in the coronary ostium throughout the maneuver
Step 4: perform controlled traction (video 1)
- Initiate slow, progressive, and strictly coaxial traction with the right hand, maintaining alignment with the vessel axis
- Apply traction in a continuous and controlled manner, avoiding abrupt increases in force
- Maintain uninterrupted fluoroscopic monitoring to assess wire behavior, stent interaction, and vessel integrity
- Avoid any jerky, rotational, or twisting movements, as these may promote guidewire elongation, unraveling, or fracture
- If resistance increases, pause and reassess before continuing to avoid excessive stress on the system
- Continue gradual traction until smooth and complete disengagement of the guidewire is achieved
Points of specific attention
- Coaxial traction is critical: misalignment increases risk of vessel injury
- Avoid excessive force: progress gradually under fluoroscopy
- Ensure firm grip on the entrapped wire; partial grip is ineffective
- Do not twist the wire during traction as torsional stress may lead to inner core fracture, coil unraveling, or further entrapment within stent struts, compromising structural integrity and control
- Stop immediately if deformation or vessel compromise is suspected
- Best used after failure of conventional techniques and before surgical referral
- Particularly useful in crushed stent or metallic entrapment scenarios
A word from the reviewer

Guidewire entrapment beneath a crushed stent is amongst one of the most anxiety-inducing complications an interventional cardiologist can encounter. While rare, its consequences — ranging from wire fracture and coronary perforation to emergency surgery — can be harmful. The authors are describing a technically logical, generally reproducible, and resource-efficient bailout strategy.
The central insight of this technique is both simple and underappreciated: conventional retrieval methods fail not merely due to mechanical obstruction, but because the guidewire’s inner core and outer coil act independently under traction.
The presented approach elegantly takes advantage of the wire’s existing structure rather than attempting to overcome it with additional intravascular hardware. The use of a standard needle holder — in general available in any catheterisation laboratory — further enhances its appeal: there is no obvious learning curve with novel equipment, no additional vascular access required, and no delay in implementation during a possibly rapidly evolving crisis.
The authors appropriately position this technique within a stepwise algorithmic framework — applied after failure of conventional methods but before surgical referral. This, in my view, is the correct clinical context.
Without ever having applied this technique personally, I strongly agree that it would be premature to deploy this technique as a first-line approach, as the mechanical clamping of the guidewire, if applied injudiciously, carries its own risk of outer coil damage or partial wire disruption.
What remains an open question to me is the technique’s performance across the spectrum of modern guidewire constructions. Polymer-jacketed wires, composite-core wires, and highly hydrophilic wires may each respond differently to external clamping, and operators should be aware that the mechanical behaviour described here may not be uniform across all wire platforms.
Similarly, the specific geometry of stent entrapment — particularly the degree of stent crush, the vessel angulation, and the length of jailed wire segment — will influence procedural success and should be factored into the risk-benefit assessment before proceeding.
In summary, this technique represents a thoughtful contribution to the interventional toolkit. This does not represent a frequently observed problemn, but when it occurs, having it in one’s cognitive toolkit may be the difference between a controlled percutaneous resolution and an emergency surgical referral. Its simplicity could be its greatest strength.
Disclosures
- Dr. Völz and Dr. Stracqualursi have no conflicts of interest to declare
Authors



2 comments
Great advice thanks. An equally if not more important issue is avoidance of wire entrapment in the first place. For example I have found it useful to apply slight traction on a side branch wire before main vessel stent deployment in order to prevent looping or curling of the wire on the outside of the stent which can predispose to wire entrapment. It is also inadvisable to leave a wire between 2 layers of stent struts during bifurcation stenting.
Hello, a very educational case. Would you also recommend to use a ‘floating wire’ to prevent deep intubation of the guiding catheter while pulling back..