92 results
PARTNER 2 at 10 years: transcatheter or surgical aortic valve replacement in intermediate-risk aortic stenosis
22 Jun 2026
At 10 years, the second-generation SAPIEN XT was associated with lower survival and higher reintervention than surgery in the randomised PARTNER 2A trial, whereas the third-generation SAPIEN 3 matched surgery in a propensity-matched registry comparison. Two analyses, one lesson: long-term outcome is defined by the valve...

Reviewer

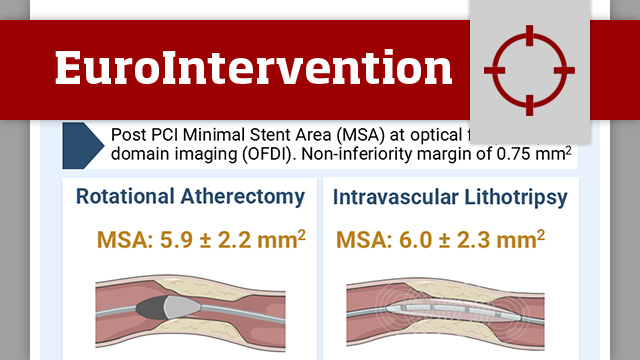
Intravascular lithotripsy in comparison to rotational atherectomy for calcified lesions: the ICARE OFDI randomised trial
01 Jun 2026
In patients with moderate-to-severe calcified coronary lesions, ICARE OFDI evaluates IVL versus rotational atherectomy as lesion preparation strategies, with OFDI-based assessment of stent results.

Reviewer
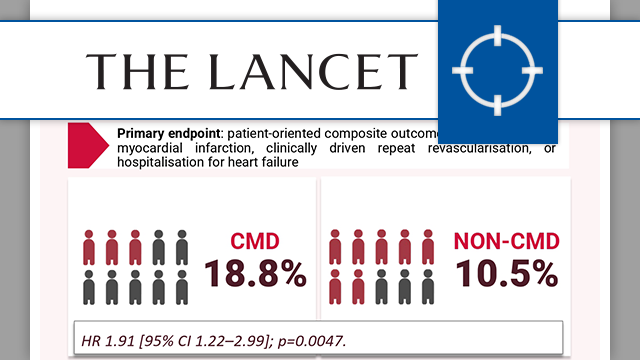
Coronary microvascular dysfunction and cardiovascular outcomes: FLOW-CMD Registry
10 Jun 2026
Coronary microvascular dysfunction is increasingly recognised as a key determinant of outcomes beyond epicardial coronary disease. The FLOW-CMD registry provides new insights into its prevalence and prognostic impact in routine invasive practice.

Reviewer

Reviewer
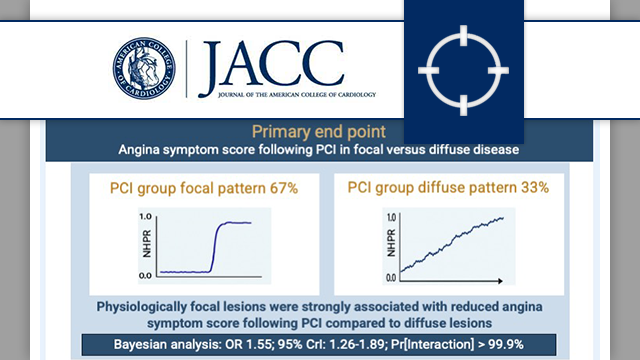
Focal and diffuse coronary artery disease patterns and placebo-controlled angina relief with percutaneous coronary intervention: ORBITA-2
09 Jun 2026
In a secondary analysis of the randomised ORBITA-2 trial, focal coronary artery disease pattern as assessed by non-hyperaemic pressure wire pullback was associated with greater angina relief following PCI than diffuse pattern of disease.

Reviewer
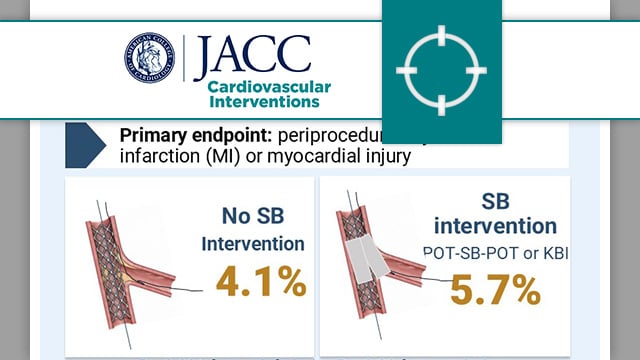
Side branch additional treatment for coronary bifurcation lesion revascularisation: insights from the KISS randomised trial
01 Jun 2026
In patients with non-left main coronary bifurcation lesions treated with provisional stenting and POT, the KISS randomised trial compares a strategy of no side branch intervention versus systematic side branch treatment.

Reviewer
Jon DeHaan Foundation and the Michele Pighi Young Investigator Awards 2026
21 May 2026
At EuroPCR 2026, two awards highlighted innovation and emerging talent in interventional cardiology. Lene Andreasen received the Michele Pighi Young Investigator Award for her research on coronary bifurcation PCI from the OCTOBER trial, while Susheel Kodali and the Nyra Medical team were honoured with the Jon...

PCR Global Interventional Academy
20 May 2026
This one-of-a-kind academy offers independent, cutting-edge training pathways for ambitious interventionalists who have been in practice for a few years and are looking to grow - both personally and professionally. Two recurrent high-level one-year tracks on coronary interventions and TAVI are already underway, with further opportunities forecast for...

Spotlight on major Late-Breaking Trials presented at EuroPCR 2026
20 May 2026
These trials were selected for their design, results, and potential to impact clinical practice: discover the key findings of an IPD meta-analysis on coronary revascularisation in TAVI patients, a long-term comparison of PCI vs. CABG for left main disease, and a study on LAA closure vs....
2026 Andreas Grüntzig Ethica Awardee: Roxana Mehran
20 May 2026
The Andreas Grüntzig Ethica Award – the highest honour in the interventional cardiology community – is presented to individuals who have contributed in an extraordinary way to the PCR mission.

EuroIntervention Case Reports has launched!
19 May 2026
The first and only peer-reviewed case report journal dedicated entirely to interventional cardiovascular medicine: EuroIntervention Case Reports.