06 Oct 2025
CLEAR-IE: outcomes of percutaneous mechanical aspiration in right-sided infective endocarditis
Selected in JACC by M. Alasnag
Can mechanical aspiration offer a safer, less invasive option for managing right-sided infective endocarditis? The CLEAR-IE registry provides valuable early insights.
References
Authors
Abdallah El Sabbagh, Benjamin Hibbert, Sripal Bangalore, Pete Fong, David Zlotnick, Bassim El-Sabawi, Robert Zhang, Brittany Zwischenberger, Ahmad Mourad, Leonard Palatnic, Sameh Sayfo, Shenise Gilyard, Stephanie Younes, Ahmad Younes, Joseph Ingrassia, Mohiuddin Cheema, Muhammad Hammadah, Anand Prasad, Nadira Hamid, Konstantinos Voudris, Pedro Villablanca, Amir Kaki, Mohammed Qintar, Zulfiqar Baloch, Marquand Patton, Alejandro Dominguez, Yasir Akhtar, Sidakpal Panaich, Nahyr Lugo-Fagundo, Evin Yucel, David O. Hodge, Kenneth Rosenfield, Larry Baddour, Paul Sorajja, John Moriarty, Sahil A. Parikh, and Sanjum S. Sethi
Reference
JACC Volume 86, Number 12
Published
27 August 2025
Link
Read the abstractReviewer

My Comment
Designed by: Mirvat Alasnag
Source: PCRonline.com
Why this study – the rationale/objective?
Transcather mechanical aspiration is an emerging technology for the management of infective endocarditis (IE), particularly of the right side. Many novel devices have been released into the global markets. Most of these devices were conceptualised for pulmonary embolism and have been integrated into algorithms for pulmonary embolism response teams (PERT).
Off-label use reported in many case reports have indicated the utility of these devices in IE. However, robust evidence on the safety and outcomes in IE is sorely lacking.
The CLEAR-IE (Cardiac Lesion Extraction and Aspiration Registry for Infective Endocarditis) is a multicenter retrospective registry of consecutive patients with right sided infective endocarditis (RSIE) undergoing percutaneous mechanical aspiration (PMA)1.
How was it executed? The methodology
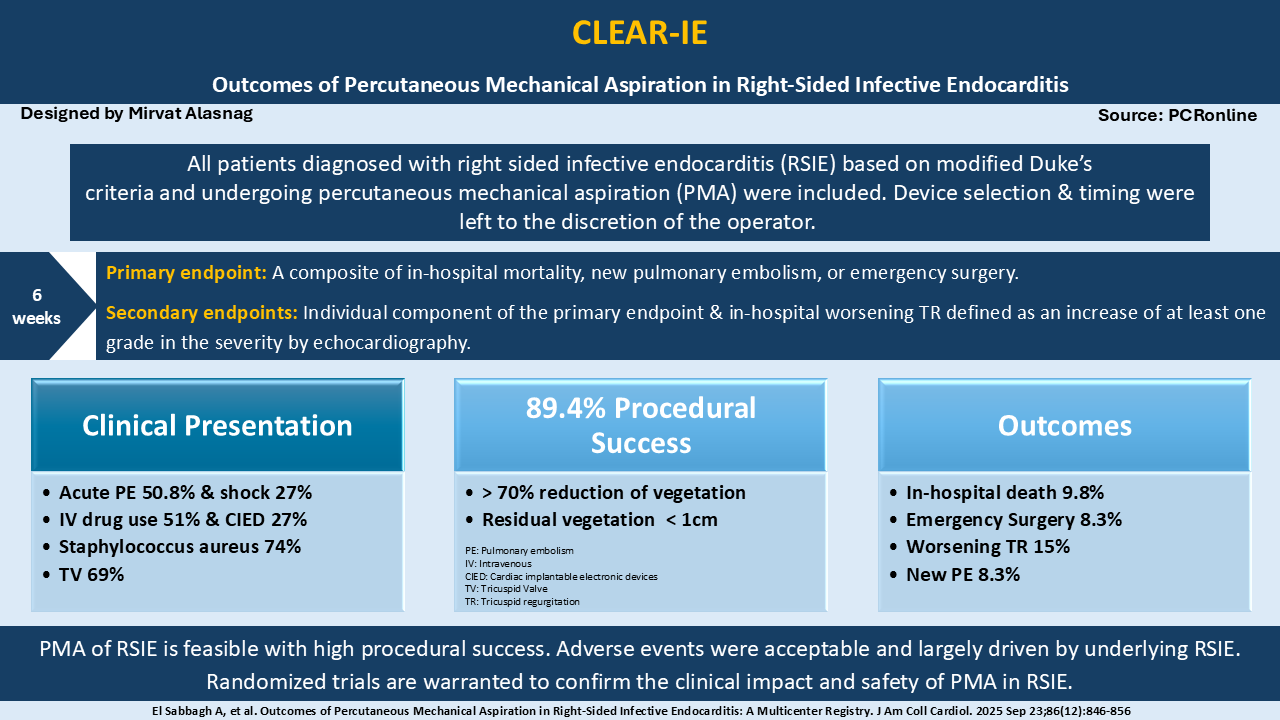
This multicenter longitudinal registry captured a broad population with right sided IE. All patients diagnosed with RSIE based on modified Duke’s criteria and undergoing right-sided PMA were included. The decision to perform PMA, device selection, clinical indication and antibiotic coverage were left to the discretion of the treating teams. Baseline characteristics such as demographics, clinical presentation, and echocardiographic features were recorded.
Procedural details included the type of aspiration device, vascular access, procedural success and complications, and post-procedure echocardiographic findings particularly worsening of tricuspid valve regurgitation (TR). In-hospital outcomes were also reported. Procedural success was defined as a > 70 % reduction in site-reported vegetation size or a residual size < 1 cm on intraprocedural echocardiography.
The primary endpoint was a composite of in-hospital mortality, new pulmonary embolism (PE), or emergency surgery. Secondary endpoints included each component of the primary endpoint and in-hospital worsening TR which was defined as an increase of at least one grade in the severity by echocardiography. The follow-up was 6 weeks, which is the universally accepted duration of antibiotic therapy.
What is the main result?
A total of 256 patients were included, of who 43 % were women. The mean age was 43 years. Implantable electronic device was reported in 27 % and intravenous drug use was reported in 51 %.
Acute pulmonary embolism was the presentation in 50.8 % of the cohort and shock in 27 %. The commonest organism identified through culture was staphylococcus aureus in 74 %. Tricuspid valve involvement was noted in 69 % with TR reported in 31 % at baseline.
The median duration of antibiotics was 8 days prior to the intervention. AngioVac was the most commonly used device (85 %). Transfemoral access was used in 53 % of the cases with the remaining being transjugular. Acute procedural success was noted in 89 %, with 64 % having residual vegetation post-aspiration.
The primary endpoint occurred in 18 % and the secondary in 9.8 %. A new PE was noted in 8.3 % with emergency surgery in 3.2 %. Right atrial endocarditis had a higher rate of success.
Critical reading and the relevance for clinical practice:
Although this is the first of its kind study, it is a retrospective analysis with no randomisation. The lack of standardised protocols and algorithms make it particularly difficult to inform practice, particularly with respect to timing and patient selection. From this analysis, we understand that women, those presenting with shock, hypoxia and right ventricular enlargement, had worse outcomes. The investigators adjusted for the different variables using multivariate analysis yet it is difficult to adjust for factors such as different device and organism. Evidence suggests that Staphylococcus aureus and enterococcus bacteremia are associated with worst outcomes2. The study included all indications such as those with electronic devices or history of drug use, which makes it very relevant. More importantly, it included a very sick population at presentation. One wonders whether a more stable cohort would have better outcomes with percutaneous aspiration?
Operator and center volume have been found to be important determinants of procedural success in other structural interventions3-5. This study did not mandate a minimum operator or center experience as the technology and approach itself remains novel and innovative. There was no core lab adjudication of the echocardiographic findings confounding the reported outcomes of residual TR and IE albeit residual TR did not appear to be a predictor of worse outcomes.
This is a large feasibility study that noted an acceptable procedural success and safety. Randomised data remain critical to understand the unique safety profile of the different devices and develop workable algorithms. Since IE requires input from multiple specialties including infectious disease and critical care experts and social workers, their input into the design of future randomised trials with a control arm.
References
- El Sabbagh A, Hibbert B, Bangalore S, Fong P, Zlotnick D, El-Sabawi B, Zhang R, Zwischenberger B, Mourad A, Palatnic L, Sayfo S, Gilyard S, Younes S, Younes A, Ingrassia J, Cheema M, Hammadah M, Prasad A, Hamid N, Voudris K, Villablanca P, Kaki A, Qintar M, Baloch Z, Patton M, Dominguez A, Akhtar Y, Panaich S, Lugo-Fagundo N, Yucel E, Hodge DO, Rosenfield K, Baddour L, Sorajja P, Moriarty J, Parikh SA, Sethi SS. Outcomes of Percutaneous Mechanical Aspiration in Right-Sided Infective Endocarditis: A Multicenter Registry. J Am Coll Cardiol. 2025 Sep 23;86(12):846-856.
- Shah ASV, McAllister DA, Gallacher P, Astengo F, Rodríguez Pérez JA, Hall J, Lee KK, Bing R, Anand A, Nathwani D, Mills NL, Newby DE, Marwick C, Cruden NL. Incidence, Microbiology, and Outcomes in Patients Hospitalized With Infective Endocarditis. Circulation. 2020 Jun 23;141(25):2067-2077.
- Mauler-Wittwer S, Noble S. Volume-Outcome Relationship in Surgical and Cardiac Transcatheter Interventions with a Focus on Transcatheter Aortic Valve Implantation. J Clin Med. 2022 Jun 30;11(13):3806.
- Bestehorn K, Eggebrecht H, Fleck E, Bestehorn M, Mehta RH, Kuck KH. Volume-outcome relationship with transfemoral transcatheter aortic valve implantation (TAVI): insights from the compulsory German Quality Assurance Registry on Aortic Valve Replacement (AQUA). EuroIntervention. 2017 Oct 20;13(8):914-920.
- Vemulapalli S, Carroll JD, Mack MJ, Li Z, Dai D, Kosinski AS, Kumbhani DJ, Ruiz CE, Thourani VH, Hanzel G, Gleason TG, Herrmann HC, Brindis RG, Bavaria JE. Procedural Volume and Outcomes for Transcatheter Aortic-Valve Replacement. N Engl J Med. 2019 Jun 27;380(26):2541-2550.

1 comment
tnx