84 results
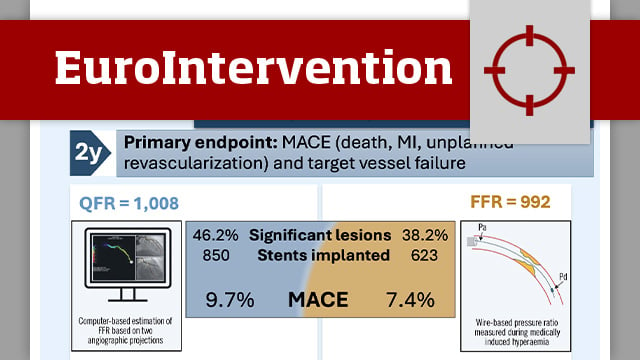
Quantitative flow ratio versus fractional flow reserve: 2-year follow-up of the FAVOR III Europe trial
06 Jul 2026
This study reports the prespecified 2-year follow-up results of the FAVOR III Europe trial, which compared quantitative flow ratio (QFR)-guided versus fractional flow reserve (FFR)-guided coronary revascularisation in patients with angiographically intermediate coronary stenoses.
FAVOR III Europe was a prospective, multicentre, randomised trial designed to evaluate whether...

Reviewer

Reviewer
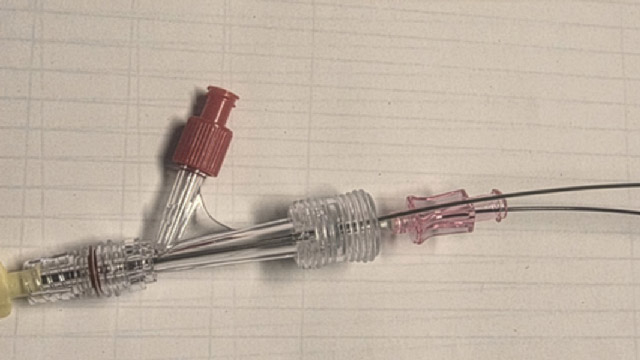
No-reflow: distal drug delivery with standard PCI equipment
23 Jun 2026
A practical guide to distal vasoactive drug delivery in no-reflow using standard PCI equipment when conventional intracoronary administration is insufficient.
Author
Author
Author
Author

Jon DeHaan Foundation and the Michele Pighi Young Investigator Awards 2026
21 May 2026
At EuroPCR 2026, two awards highlighted innovation and emerging talent in interventional cardiology. Lene Andreasen received the Michele Pighi Young Investigator Award for her research on coronary bifurcation PCI from the OCTOBER trial, while Susheel Kodali and the Nyra Medical team were honoured with the Jon...

PCR Global Interventional Academy
20 May 2026
This one-of-a-kind academy offers independent, cutting-edge training pathways for ambitious interventionalists who have been in practice for a few years and are looking to grow - both personally and professionally. Two recurrent high-level one-year tracks on coronary interventions and TAVI are already underway, with further opportunities forecast for...

2026 Andreas Grüntzig Ethica Awardee: Roxana Mehran
20 May 2026
The Andreas Grüntzig Ethica Award – the highest honour in the interventional cardiology community – is presented to individuals who have contributed in an extraordinary way to the PCR mission.

PCR Fellowship Programmes: A new international stepping stone in PCR’s educational universe
19 May 2026
PCR has developed an independent educational framework to facilitate the worldwide training of the next generation of interventional cardiologists in host centres that are renowned for their expertise. This new initiative supports practitioners at all stages of their career – promoting professional growth, geographical mobility and cultural exchange.

ViTAL®: Visionary Transformative Adult Learning – The Manual
19 May 2026
ViTAL® (Visionary Transformative Adult Learning) was born from a simple but demanding conviction: experienced professionals continue to learn best through interaction, reflection, shared experience, and active participation.

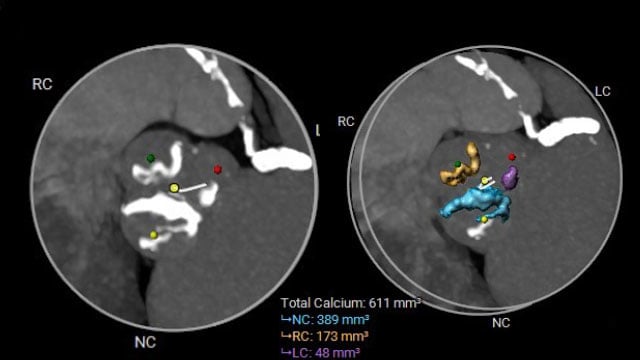
High calcium, high stakes: managing severe AS with complex multivessel disease
12 May 2026
A 69-year-old woman with severe symptomatic aortic stenosis (NYHA III) and complex comorbidities, including three-vessel coronary artery disease, advanced COPD, and peripheral artery disease, presents with progressive dyspnoea despite recent PCI. How would you treat this patient?

Author

Author

Author
Eugene Braunwald: the world of cardiology and medicine mourns the loss of one of its greatest practitioners
24 Apr 2026
Eugene Braunwald, whose work reshaped cardiovascular medicine into the rigorous, evidence-based discipline we know today, leaves behind an extraordinary scientific legacy. He transformed how we think about the heart: not just as an organ to observe, but as a system to understand, measure, and treat through...

Self-made steerable catheter to cross the aortic valve in severe aortic stenosis
15 Apr 2026
When standard catheters and wires repeatedly fail to cross a severely stenotic aortic valve, a simple modification of readily available equipment may provide a solution.
This step-by-step tutorial explains how to create and use a self-made steerable catheter system to facilitate valve crossing in complex TAVI anatomies.
Author
Author

Author