223 results
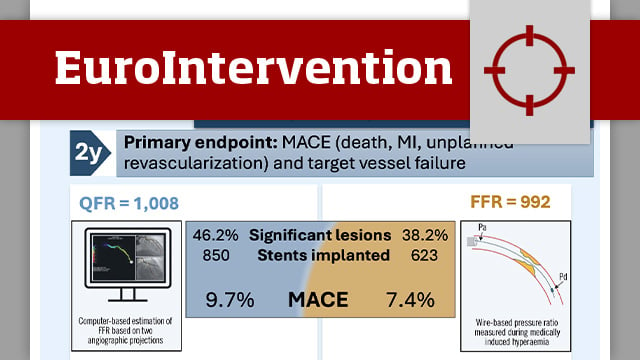
Quantitative flow ratio versus fractional flow reserve: 2-year follow-up of the FAVOR III Europe trial
06 Jul 2026
This study reports the prespecified 2-year follow-up results of the FAVOR III Europe trial, which compared quantitative flow ratio (QFR)-guided versus fractional flow reserve (FFR)-guided coronary revascularisation in patients with angiographically intermediate coronary stenoses.
FAVOR III Europe was a prospective, multicentre, randomised trial designed to evaluate whether...

Reviewer

Reviewer
PARTNER 2 at 10 years: transcatheter or surgical aortic valve replacement in intermediate-risk aortic stenosis
22 Jun 2026
At 10 years, the second-generation SAPIEN XT was associated with lower survival and higher reintervention than surgery in the randomised PARTNER 2A trial, whereas the third-generation SAPIEN 3 matched surgery in a propensity-matched registry comparison. Two analyses, one lesson: long-term outcome is defined by the valve...

Reviewer

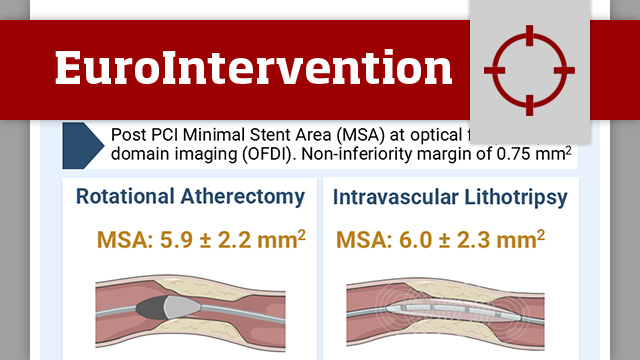
Intravascular lithotripsy in comparison to rotational atherectomy for calcified lesions: the ICARE OFDI randomised trial
01 Jun 2026
In patients with moderate-to-severe calcified coronary lesions, ICARE OFDI evaluates IVL versus rotational atherectomy as lesion preparation strategies, with OFDI-based assessment of stent results.

Reviewer
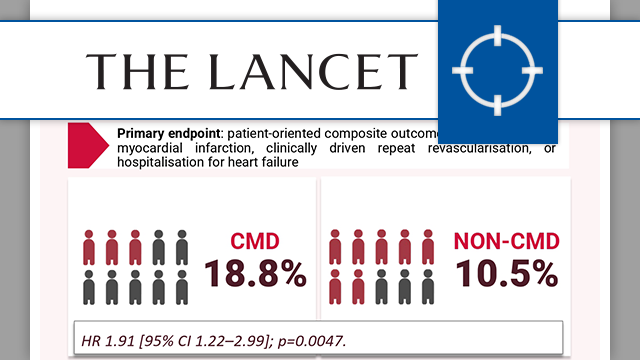
Coronary microvascular dysfunction and cardiovascular outcomes: FLOW-CMD Registry
10 Jun 2026
Coronary microvascular dysfunction is increasingly recognised as a key determinant of outcomes beyond epicardial coronary disease. The FLOW-CMD registry provides new insights into its prevalence and prognostic impact in routine invasive practice.

Reviewer

Reviewer
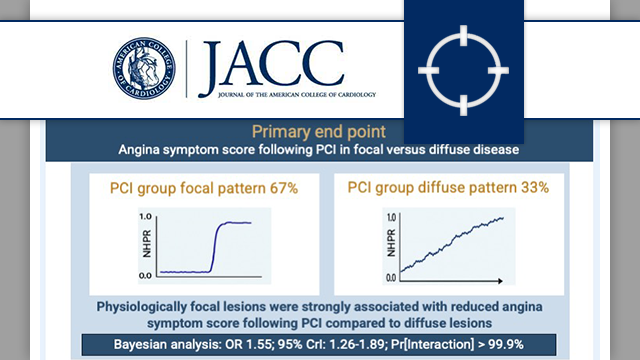
Focal and diffuse coronary artery disease patterns and placebo-controlled angina relief with percutaneous coronary intervention: ORBITA-2
09 Jun 2026
In a secondary analysis of the randomised ORBITA-2 trial, focal coronary artery disease pattern as assessed by non-hyperaemic pressure wire pullback was associated with greater angina relief following PCI than diffuse pattern of disease.

Reviewer
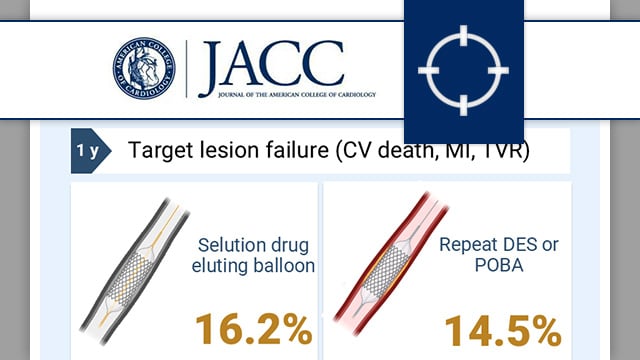
Sirolimus-eluting balloon vs. repeat drug-eluting stent or balloon angioplasty for coronary in-stent restenosis
03 Jun 2026
In-stent restenosis remains the Achilles heel of PCI. Drug-eluting balloons offer a potential strategy for the treatment of in-stent restenosis. To date, implantation of a further drug-eluting stent provide better long-term outcomes compared to paclitaxel drug-eluting balloons.
In this trial, the authors compare the safety and efficacy...

Reviewer

Reviewer
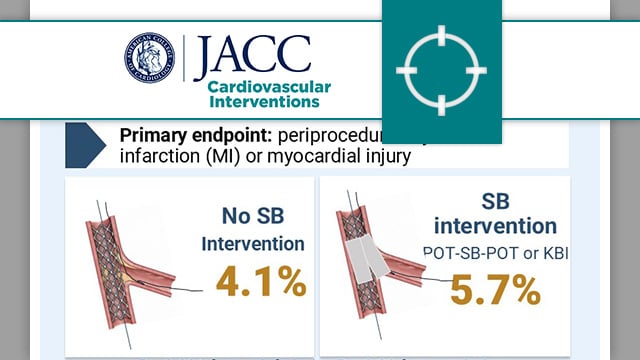
Side branch additional treatment for coronary bifurcation lesion revascularisation: insights from the KISS randomised trial
01 Jun 2026
In patients with non-left main coronary bifurcation lesions treated with provisional stenting and POT, the KISS randomised trial compares a strategy of no side branch intervention versus systematic side branch treatment.

Reviewer
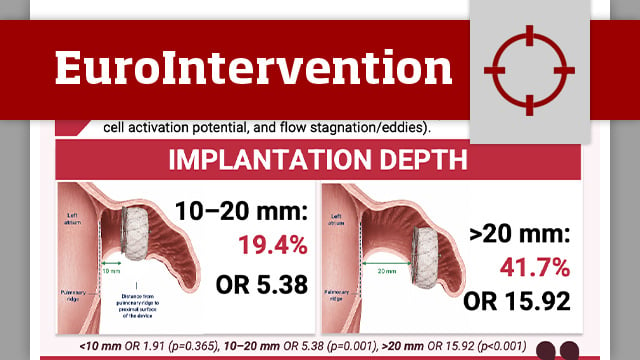
Impact of device implantation depth on blood flow dynamics after left atrial appendage closure
28 Apr 2026
The study aimed to evaluate the impact of LAAC device implantation depth on local flow characteristics and its association with device-related thrombus using patient-specific computational fluid dynamics.
Reviewer
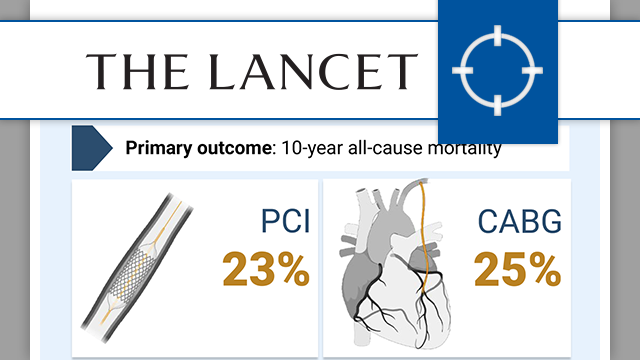
NOBLE trial: 10-year outcomes of PCI vs CABG in left main disease
13 Apr 2026
Long-term evidence comparing PCI and CABG for unprotected left main coronary disease has been limited and sometimes conflicting. The 10-year results from the NOBLE trial now provide important clarity on all-cause mortality outcomes with both revascularisation strategies.

Reviewer
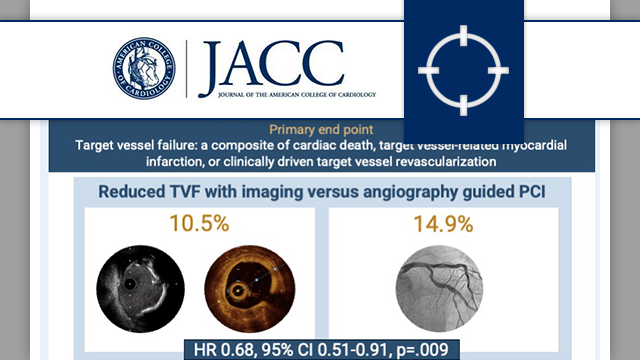
Intravascular imaging vs angiography guided complex PCI: 5-year outcomes from a randomised trial
13 Apr 2026
The RENOVATE-COMPLEX-PCI 5-year outcomes confirm the long-term durability of benefits seen with intracoronary imaging over angiography guided PCI in complex lesions.
Reviewer

Reviewer