03 Jun 2024
Prehospital crushed versus integral prasugrel loading dose in STEMI patients with a large myocardial area
Selected in EuroIntervention by L. Koliastasis
This pre-specified substudy of CompareCrush aimed to examine if patients with a large myocardial infarction benefit from prehospital crushed prasugrel.
References
Authors
Jeroen M. Wilschut; Rosanne F. Vogel; Jacob J. Elscot; Ronak Delewi; Miguel E. Lemmert; Nancy W.P.L. van der Waarden; Rutger-Jan Nuis; Valeria Paradies; Dimitrios Alexopoulos; Felix Zijlstra; Gilles Montalescot; Dominick J. Angiolillo; Mitchell W. Krucoff; Pieter C. Smits; Georgios J. Vlachojannis; Nicolas M. Van Mieghem; Roberto Diletti
Reference
DOI: 10.4244/EIJ-D-23-00618 • APR 1, 2024
Published
1 April 2024
Link
Read the abstractReviewer

My Comment
Pre-specified substudy of the CompareCrush Trial.
Courtesy of Leonidas Koliastasis. Source: PCRonline.com
Why this study – the rationale/objective?
The CompareCrush randomized trial demonstrated that pre-hospital loading dose with crushed prasugrel was not clinically beneficial compared to integral tablets. However, the effect of pre-treatment with crushed prasugrel pre-hospital in STEMI patients with large myocardial area at jeopardy is not known.
This pre-specified substudy of CompareCrush aimed to examine if patients with a large myocardial infarction benefit from prehospital crushed prasugrel.
How was it executed – the methodology?
The CompareCrush study randomised 633 patients to receive either crushed or integral prasugrel 60 mg loading dose alongside 500 mg of aspirin and 5000 IU of heparin in the ambulance once a STEMI was diagnosed.
This pre-specified sub-study includes 532 patients with ambulance 12 lead ECG available. Patients were stratified into two groups according to pre-hospital myocardial area at risk. Large area at risk was defined as cumulative ST-segment deviation of > 15 mm.
The endpoints included:
- Early myocardial reperfusion parameters TIMI 3 flow, high thrombus burden (TIMI thrombus grade ≥ 3, myocardial blush grade 3 (pre and post procedure)
- Clinical outcomes (all-cause mortality, myocardial reinfarction, stent thrombosis, IIb/IIIa bailout administration, stroke and urgent revascularization).
What is the main result?
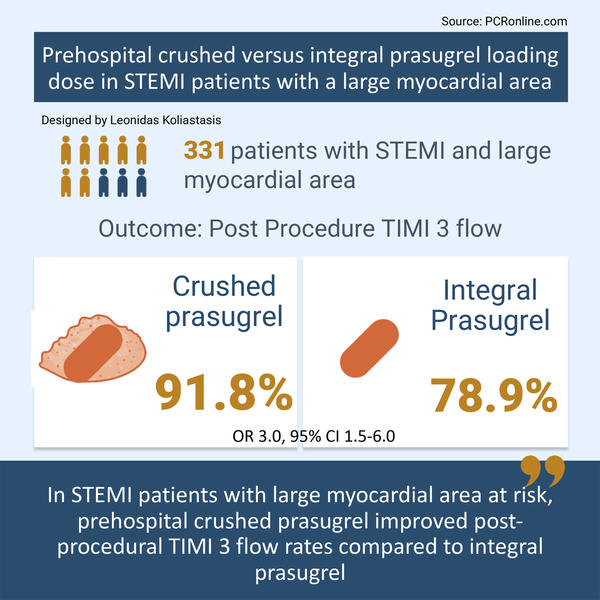
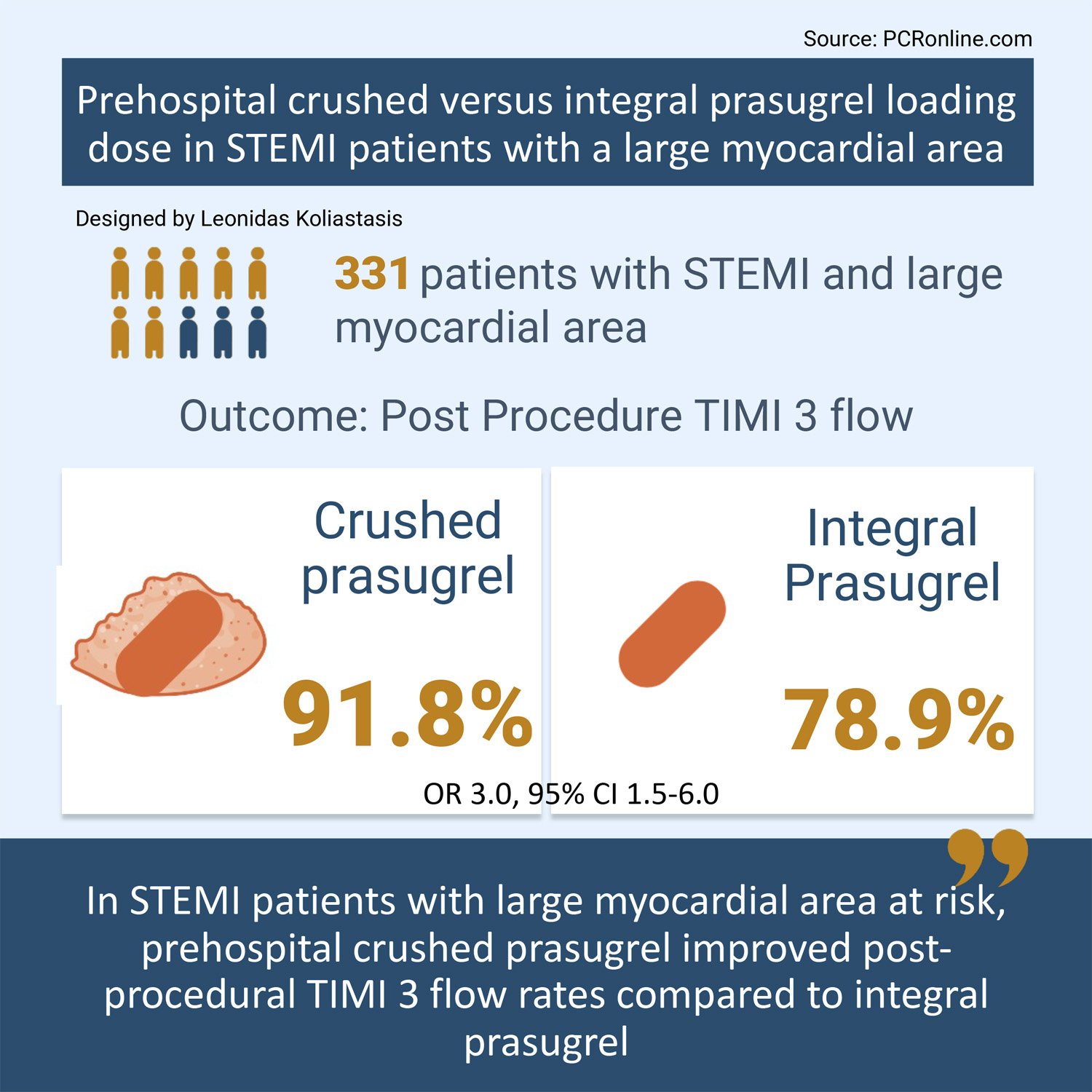
Of the 532 patients with available ambulance ECGs 331 (62 %) had a large myocardial area at jeopardy. In both the large myocardial area at risk group and non-large, 52 % of patients received crushed prasugrel loading dose. LAD occlusion was more common in patients with large area at risk (46 % vs 31 %; p = 0.001) with the remaining characteristics were well balanced.
- In the large myocardial area at risk group pre-procedural TIMI 3 flow (OR 0.56, 95 % CI: 0.38-0.82) and high thrombotic burden (OR 1.80, 95 % CI: 1.13-2.87) were more common.
- Post-procedural TIMI 3 flow was lower in the large myocardial area at risk group (86 % vs. 93 %, OR 0.46, 95 % CI 0.24-0.88, p = 0.019)
- Crushed prasugrel significantly increased the rate of post-procedural TIMI 3 flow in patients with large myocardial area at risk group (crushed: 92 % vs integral: 79 %, OR 3.00, 95 % CI: 1.50-6.00).
Critical reading and the relevance for clinical practice
This subgroup analysis of the CompareCrush trial showed that pre-hospital loading dose of crushed prasugrel led to higher rates of post-procedural TIMI III flow in patients with large myocardial area at risk. Suboptimal flow after PCI is associated with worse clinical outcomes and larger final infarct size, therefore, crushed prasugrel may offer an effective and cost-effective strategy in this patient group. An important caveat to this pre-specified substudy is that the CompareCrush trial failed to meet its primary endpoint ,therefore all analysis in this paper are hypothesis generating.
The CompareCrush trial demonstrated that crushed prasugrel leads to more potent platelet inhibition, however, that was not translated into improved angiographic, procedural or clinical outcomes. In this substudy, a simple ECG-based pre-hospital analysis was used to identify large myocardial area at-risk.
In the large infarction group, crushed prasugrel improved the incidence of post-intervention TIMI III flow. The remaining angiographic endpoints were similar, with crushed and integral prasugrel as were the clinical endpoints. In the non-large infarction group, there were no differences in any of the angiographic or clinical endpoints between crushed and integral prasugrel.
The strengths of this analysis include the prespecified protocol, the blinded core lab analysis of the angiographic parameters and the independent clinical events adjudication. The interventions of crushing prasugrel and ECG analysis for large infarction classification ar both simple and low-cost interventions.
There are important in-built limitations to the substudy, including the lack of power and whilst characteristics were well balanced between groups, randomization was not stratified by large versus non-large MI. Furthermore, it is possible that ECG lacks sensitivity and/or specificity to distinguish large myocardial area at risk in comparison to enzymic progression or cardiac magnetic resonance imaging.
Overall, in STEMI patients with large myocardial area in jeopardy, crushed prasugrel pre-hospital loading dose administration may be a beneficial strategy, however, this confirmatory randomised trials in this population.
References
- Wilschut JM, Vogel RF, Elscot JJ, Delewi R, Lemmert ME, van der Waarden NWPL, Nuis RJ, Paradies V, Alexopoulos D, Zijlstra F, Montalescot G, Angiolillo DJ, Krucoff MW, Smits PC, Vlachojannis GJ, Van Mieghem NM, Diletti R. Prehospital crushed versus integral prasugrel loading dose in STEMI patients with a large myocardial area. EuroIntervention. 2024 Apr 1;20(7):e436-e444. doi: 10.4244/EIJ-D-23-00618.
- Vlachojannis GJ, Wilschut JM, Vogel RF, Lemmert ME, Delewi R, Diletti R, van der Waarden NWPL, Nuis RJ, Paradies V, Alexopoulos D, Zijlstra F, Montalescot G, Angiolillo DJ, Krucoff MW, Van Mieghem NM, Smits PC. Effect of Prehospital Crushed Prasugrel Tablets in Patients With ST-Segment-Elevation Myocardial Infarction Planned for Primary Percutaneous Coronary Intervention: The Randomized COMPARE CRUSH Trial. Circulation. 2020 Dec 15;142(24):2316-2328. doi: 10.1161/CIRCULATIONAHA.120.051532.
2 comments
Not new, US ER’s have been instructing EMT runs to administer crushed Prasugrel or Ticagrelor to AMI’s for years, but enthusiasm tempered more recently by increased bleeding. Probably best answer is to forego this approach and use IV Cangrelor immediately on hospital arrival — a trial should be initiated !!
its costeffective strategy but need more data ; one can chew if taste of tablet not too bitter