19 Dec 2019
Undilatable calcific lesion even after rotational atherectomy
Euro4C Case
View this very uncommon case in which balloons do not expand even after a rather aggressive rotational atherectomy: a 43-year-old male with hypertension, smoking and dyslipidemia presents with total occlusion of proximal left anterior descending artery with fresh thrombus...

Authors


Let’s exchange opinions on this case. This could happen to you tomorrow…
Clinical presentation
- A 43 yo Male
- Risk factors: arterial hypertension, smoking, dyslipidemia
- Clinical presentation: chest pain with irradiation to both arms and dyspnea
- ECG: antero-lateral STEMI

Primary PCI
Post aspiration thrombectomy and PCI with DES implantation was performed from the left radial approach
Non-culprit: right coronary artery
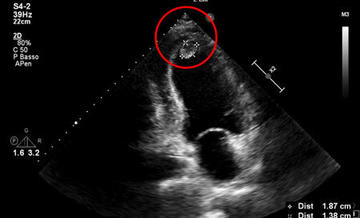
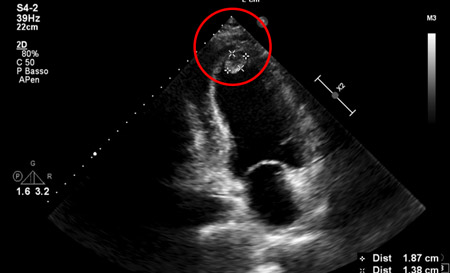
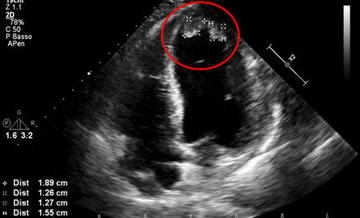
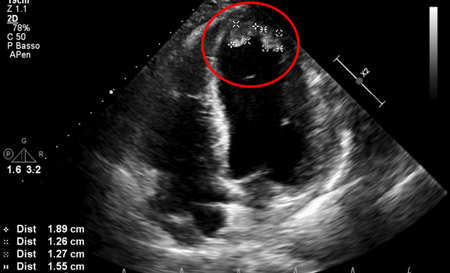
Post STEMI TTE shows akinesia of the apex with thrombus formation. Anticoagulation with heparin initiated.
Given the young age, PCI before discharge was chosen
Lesions were crossed with a BMW wire and multiple dilatations with NC balloons and cutting balloon were attempted, but significant ‘‘dog-boning" of the balloons persisted.




Then, rotational atherectomy with 1,50 mm burr first, and then with a 1,75 mm burr (Rotapro) were performed from the same 6F radial approach.
However, even after RA NC balloon at 24 atm and cutting balloon at 20 atm did not expand.
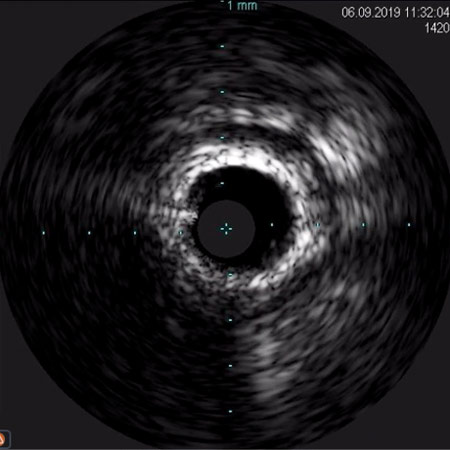
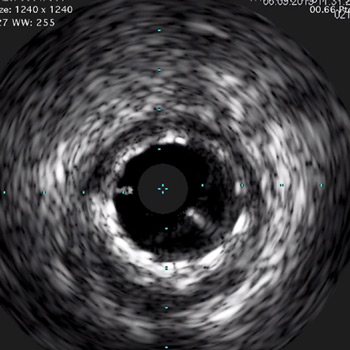
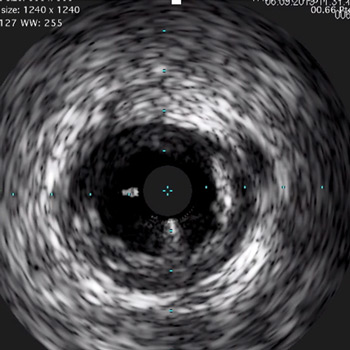
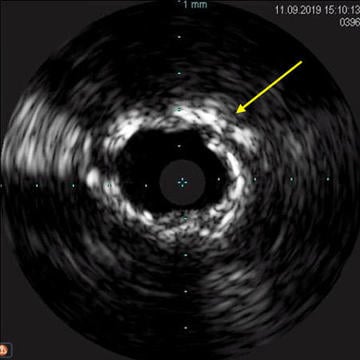
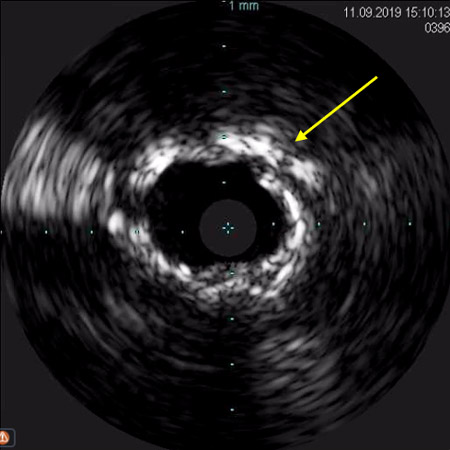
IVUS clearly showed undilatable calcific lesion at the mid-segment of the RCA. Stenting distal right coronary segment with good expansion
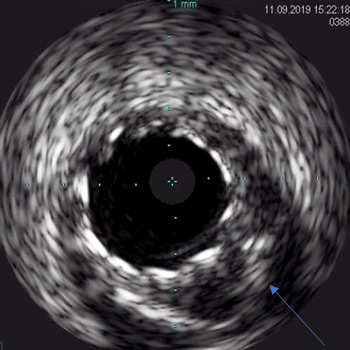
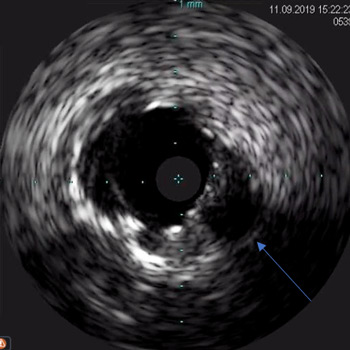
IVUS assessment in detail
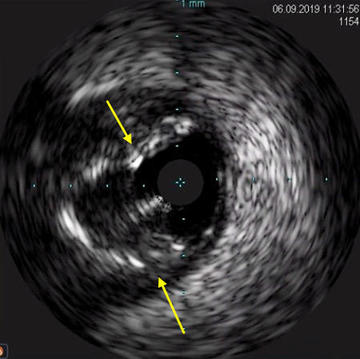
Localized dissection in the proximal segment
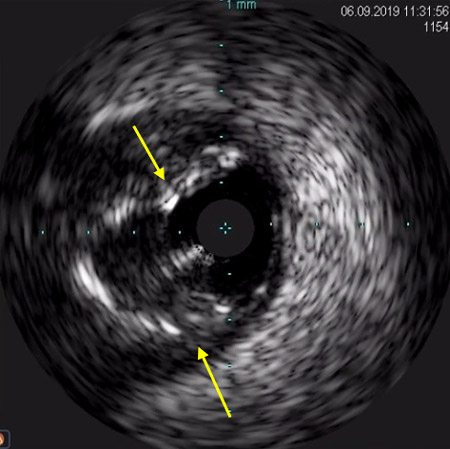

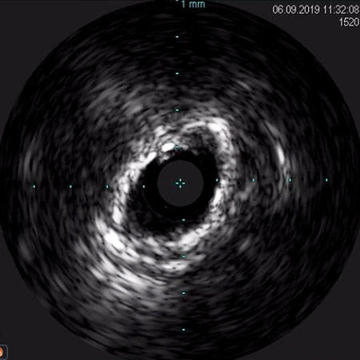
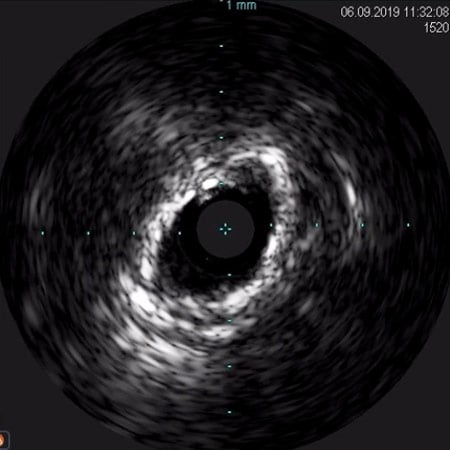
Non-fractured circumferential calcification
Non-fractured circumferential calcification
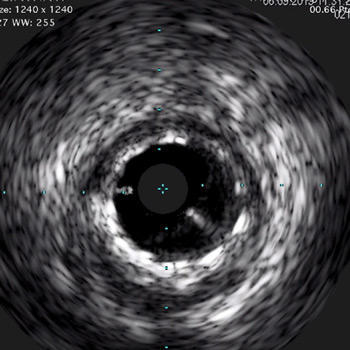
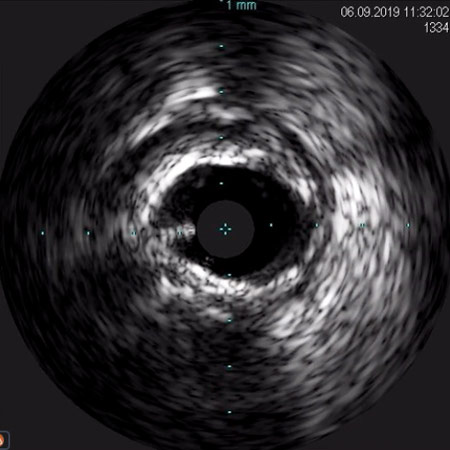
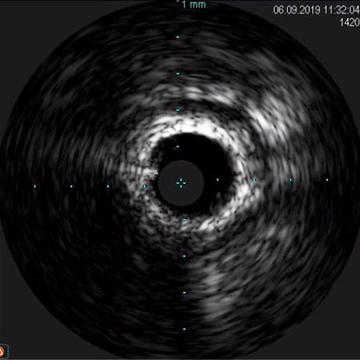
Distal stent

Distal vessel
How would I treat?
- Upgrade to a 2.0mm burr? (in this case the 6Fr guiding catheter from the radial artery is not compatible).
- Try even higher balloon pressures…?
- Try a lithotripsy balloon…?
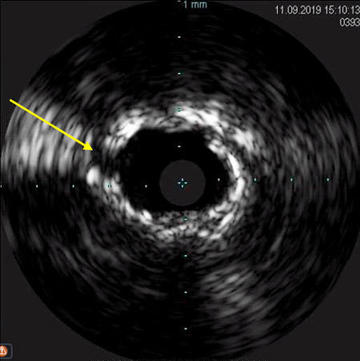
Intravascular lithotripsy (IVL) with 4-mm Shockwave balloon: a full balloon expansion was achieved after three cycles of IVL.
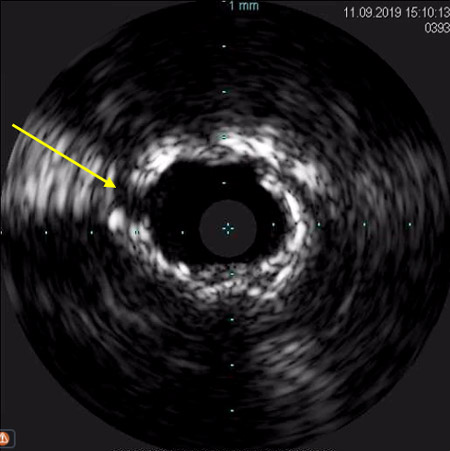
Intravascular ultrasound (IVUS) showing adequate plaque modification (arrows point at calcium fractures).
Final result after stenting of proximal and mid RCA segments
IVUS shows and «almost ruptured» artery wall (arrows)
IVUS shows and «almost ruptured» artery wall (arrows)
Considerations on this case
- Resistant, calcified fibro-calcific lesions can be found even in very young patients
- This is a very infrequent case in which balloons do not expand even after a rather aggressive RA (burr/artery ratio >0.5)
- Probably larger RA burr might have allowed balloon expansion, but the availability of the new lithotripsy technology appeared indicated once a rather large MLD had been created by the RA burrs. Indeed, the lithotripsy balloons can cross only lesions with relatively large MLD after expansion of the tight coronary lumen
- The lithotripsy balloon was very effective in achieving the plaque rupture and allowed easy stent expansion with good final result as assessed by IVUS
- The final angiogram shows a damaged arterial wall (arrow) due to the aggressive treatment.
- Further expansion might have caused a large artery rupture…
Medical therapy and follow-up
- Due to the apical thrombosis, the patient was discharged on triple anti-thrombotic therapy (Warfarin, aspirin and ticagrelor, the later maintained after primary PCI given the young age and low bleeding risk).
- The apical thrombus disappeared at a 3-month echographic control and the EF reached 40%.
- DAPT was indicated for 12 months.
"Thank you all for your comments.
The enthusiasm and the different points of view raised in the discussion witness the interest that this kind of “daily life” case may arise among the community.
Indeed, there might be different ways to solve the problem of an undilatable lesion even after RA (a larger burr, highest pressure with balloons, IVL), and we know that there is no "scientific evidence” in support of one or other strategy.
The one we choose was an option that worked and our case suggests that RA and IVL may be complementary strategies rather than competitive options.
Your suggestion of a long-term follow-up is a good one and we will try to do it; so, keep tuned and we will share this with you by the end of 2020.
Now, get ready for the next Euro4C case…. this could happen to you tomorrow…"
Flavio Ribichini for Euro4C


12 comments
Congratulations Flavio and Concetta for sharing this case with excellent iconography. Had a similar case in a 48yo man with similar risk profile. This is an ideal indication for a lithotripsy balloon (that is definitely compatible with a 6F guide) because the residual concentric calcific ring is very focal. It is unlikely that a bigger burr would ablate sufficiently the residual amount of calcium because the contact between the burr and the vessel would not be enough and the residual stenosis is not so tight. No experience with ELCA that might be an option. My take-home message is that RA and intravascular lithotripsy are very complementary devices for optimal procedural and long-term outcomes.
PANAGIOTIS PETROPOULAKIS IVL is the only option to do this safely.
Congratulation and thank you for sharing this interesting case with us. In my opinion the real question for significant number of us would be "what if IVL is not available in your country?".
I would go for Lithotripsy balloon
Dear Flavio, excellent case presenting a classical challenge. Calcified ring, Rota 1,75mm insufficient. Of Course there are almost 3 options: 1. OPNC 35 atm 2. IVL 3. Change to 8F and 2,15 mm Burr My preferred strategy will be nr. 3. For 1 and 2 data is limited. Risk of Perforation is lowest with rota. If rota is good, more rota is better! Best regards, Markus
Nice and surprising case in a patients whose age would not raise suspect about such a severe calcification. I also would have performed the PCi before discharge. Otherwise, with the requirement of oral anticoagulation due to the presence of thrombus in the LV, the logistic would be more difficult. In my opinion and despite we still not have lithotripsy balloon, the results of this device makes it really adequate to sort out this case. The other option, which would be the one possible in our center would be to the change the sheath with the 7 French Glidesheath slender of Terumo, which allows to use a 7F guiding catheter and use a 2.0 mm burr, although I am not sure that the ablation with that size will be enough. Fortunately, lithotripsy will be available soon.
Very interesting case. After RA with 1.75 burr I think a good option could be lithotripsy balloon. If it wouldn't cross the lesion I would try with laser
Congratulation Flavio for the excelent managment of the patient, and for very clear demonstration of your strategy! This case also testifies for the fact that Rota and shockwave are complementary rather than competitive. Regards, Marko (Noc)
Congratulations for the case. We have had a couple of similar cases that let us learn that Rotational atherectomy (RA) and IVL are complementary tools. Specially when deep calcium exist, RA could not be able to fracture the plaque and permit complete balloon expansion. Thus, intracoronary imaging, as was done in this case is a key point to understand what kind of lesion we are facing and if IVL could be the best option. On the other hand, some of these lesions produces critical stenosis that precludes delivery of Shockwave balloon, and the only way to do it is to perform RA previously. Congrats again and thank you for sharing! #Rotatripsy
Congratulations to Flavio for the excellent management of this complex case. One more option in case of undilatable lesion, before performing the more expensive lithotripsy, is to try the ultra high pressure OPN balloon from SIS medical. But, sometimes, lithotripsy is the final solution. This is something from our experience: Venuti G, D'Agosta G, Tamburino C, La Manna A. Coronary lithotripsy for failed rotational atherectomy, cutting balloon, scoring balloon, and ultra-high-pressure non-compliant balloon. Catheter Cardiovasc Interv. 2019;94(3):E111–E115. doi:10.1002/ccd.28287
Excellent case. I also believe it would be very interesting to know the long-term follow-up due to the image of almost rupture of the artery wall. Lithotripsy is still a new technique and our experience is limited. If it were possible to perform angiographic follow-up with ultrasound it would be fantastic. Probably the outcome will be optimal, but we should take advantage of these cases to improve our knowledge.
In my practice, rotational atherectomy would have been the first-line strategy as well. However, it is clear from the angiographic and IVUS images after the 1.75 mm burr and the failed dilatation with NC and cutting balloons, that the 1.75 mm burr could not even reach the arterial wall, which is the actual mode of failure (it is not a super-resistant calcified plaque). Therefore, the burr-to-artery ratio utilized is not >0.5 as detailed in the take-home messages, whereas quite less (in fact, a 4-mm Shockwave balloon was used). Probably, the plaque would have been modified adequately with a 2.00-mm burr, which would have been also more cost-effective than adding a Shockwave balloon to the final invoice. Anyway, I also appreciate that switching to a 2.00-mm burr would have required changing guide catheter and sheath, and probably an IVL-based strategy more quickly achieved the nice final result.