PCI for in-stent restenosis complicated by neoatherosclerosis dissection
#CardioTwitterCase originally published on Twitter
Did you know that neoatherosclerosis (in the context of in-stent restenosis (ISR)) can suffer dissection, just like any native coronary artery, when balloon dilatation is performed?
This case was originally published on Twitter by @LAzzaliniMD
Case description
This is a 68-year-old man with ischemic cardiomyopathy (LVEF 25 %), end-stage renal disease on dialysis, and history of multiple previous PCIs with stents in the RCA, LCx, LAD and LM, who presented with angina during dialysis sessions.
Coronary angiogram showed ISR at the LM bifurcation, as well as in the mid LAD. Balloon dilatation of the LM bifurcation was performed successfully and uneventfully. After balloon dilatation of the mid LAD ISR, however, there was abrupt vessel closure.
The differential diagnosis included: thrombosis, no reflow, and dissection. The activated clotting time (ACT) was therapeutic throughout the intervention, which made thrombosis less likely. Up to 120 µg of intracoronary epinephrine were administered in the LAD via a Sasuke dual lumen catheter, with no improvement of the flow down the LAD, which made no reflow less likely.
However, extensive dilatation of the LAD ISR with a 3.0 and a 2.5 mm NC balloon did not improve the situation either.
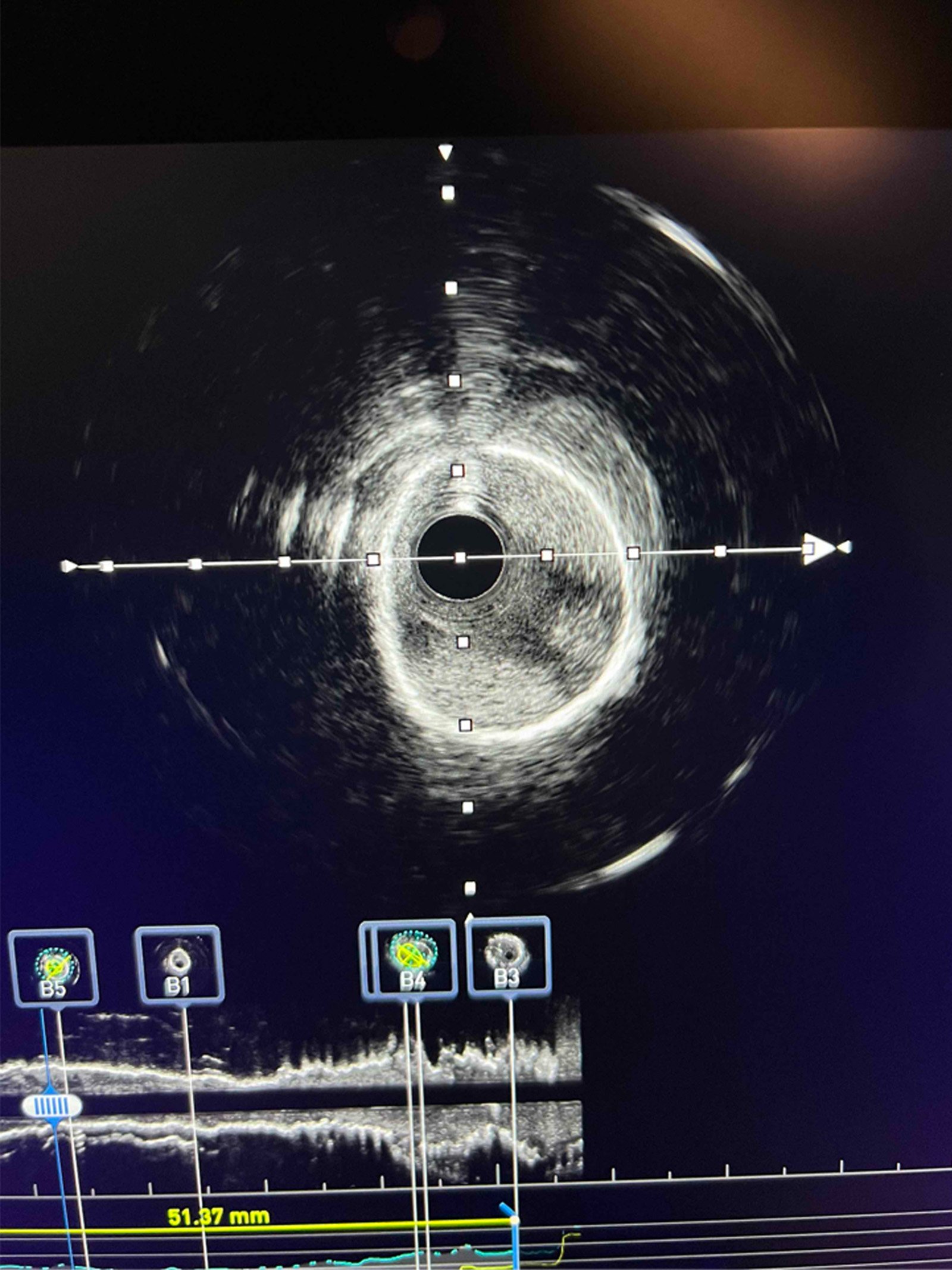
Therefore, a pull-back injection of contrast via the Sasuke dual lumen catheter from the distal to the proximal LAD was performed, which highlighted an area of tight stenosis and haziness in the mid LAD ISR. IVUS was performed and confirmed the presence of dissection within what appeared neoatherosclerotic tissue at that level.
A new stent (3.5 x 16 Synergy Megatron) was implanted and postdilatetd with a 3.5 mm NC balloon, with re-establishment of TIMI 3 flow down the LAD.
The patient was discharged uneventfully 4 days later.
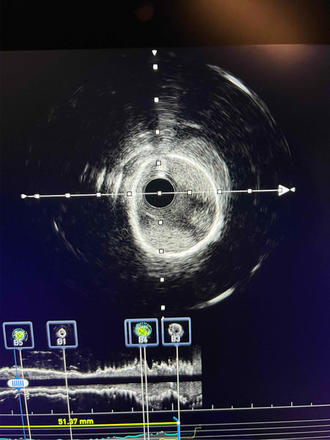
IVUS showing neoatherosclerosis with neointimal dissection
Videos
Final remarks
In-stent restenosis with neoatherosclerotic tissue in the context of ISR can suffer dissection upon balloon dilatation, just like a native coronary artery. In such cases, and when coronary flow is impaired, stenting is warranted.
Original tweet and Twitter discussion
You are performing #PCI on the following case of diffuse #ISR.
— Lorenzo Azzalini (@LAzzaliniMD) April 17, 2024
You balloon , and this result is observed : pic.twitter.com/zkDYq0n9FF
Author



No comments yet!