02 Jul 2024
Supplementary super-high pressure balloon-based plaque modification after intravascular lithotripsy
#CardioTwitterCase originally published on Twitter
Additional balloon-based plaque modification after ineffective intravascular lithotripsy of a heavily calcified ostial CX
This case was originally published on Twitter by @KambisMashayek1
Case description
A 69-year-old diabetic male patient presented with angina and dyspnea on moderate exertion for about 6 months. His past medical history included three-vessel coronary artery disease with previous PCIs in the RCA, LAD and left main (LM). Echocardiography findings showed a preserved left ventricular ejection fraction.
Coronary angiogram revealed severely calcified, significant stenosis of the ostial CX, and sufficient angiographic result after provisional stenting of the LM and LAD 9 years ago (Videos 1 and 2). The detailed calcium pattern showed an excentric and very thick calcification just on the ostium of the CX, visualized by high-frame and high-resolution angiography.
Based on these findings, intravascular lithotripsy with a 3.5 mm Shockwave balloon was used to facilitate plaque modification. After 80 pulses, a dog-bone effect was still documented (Video 3). Angiography showed an acceptable plaque modification result without any dissection after intravascular lithotripsy (Video 4). Additional dilatation with a 3.5 mm non-compliant balloon at 26 atmospheres divulged further persistent balloon under-expansion (Video 5). Furthermore, the complementary use of a 3.5 mm super-high pressure balloon (OPNC SIS Medical), inflated initially up to 35 (Video 6), and finally up to 45 atmospheres, led to an adequate balloon expansion (Video 7).
A reverse culotte stenting technique with additional stent implantation (Onyx Trucor 3.5 x 18 mm) from LCX to LM was adopted after the mentioned extended lesion preparation (Figure), followed by POT, kissing balloon and final re-POT with a 4.5 mm non-compliant balloon. An excellent angiographic result with TIMI 3 and adequate stent expansion was achieved (Videos 8 and 9). The patient was discharged uneventfully the next day.
Videos
Figure
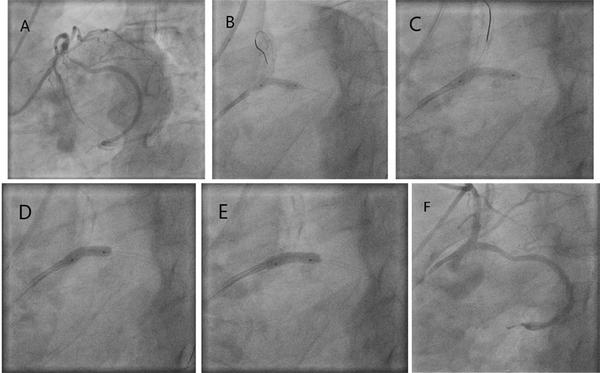
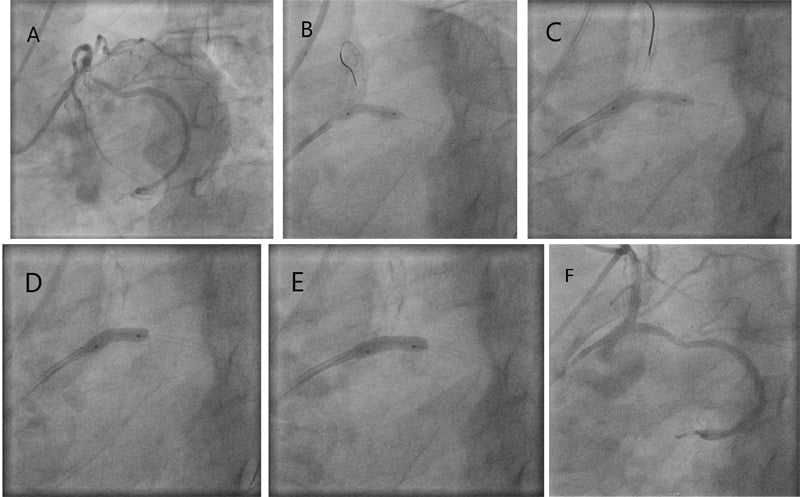
Figure: Summary of the ostial CX procedure.
A. Heavily calcified stenosis of the ostial CX.
B. Final result after intravascular lithotripsy with 3.5 mm Shockwave balloon.
C. Additional dilatation with 3.5 mm non-compliant balloon at 26 atmospheres.
D. Super-high pressure balloon (OPNC SIS Medical) inflated initially up to 35 atmospheres.
E. Super-high pressure balloon (OPNC SIS Medical) inflated initially up to 45 atmospheres.
F. Final angiographic result after intravascular lithotripsy, super-high pressure balloon, and reverse culotte stenting technique.
Final remark
Super-high pressure balloon angioplasty can be an efficient supplementary bailout strategy after insufficient plaque modification with intravascular lithotripsy in cases of heavily calcified lesions and insufficient lesion preparation prior to stent implantation.
Original tweet and Twitter discussion
Combination of IVL- @ShockwaveIVL and OPNC @sis_medical are often used as complementary tools for better outcome. IVL modifies the thick calcified plaque, OPNC compresses the plaque resulting in optimal outcome. @OPCILive@PCRonline@CtoEuro@MLCTOAcademy@incathlabpic.twitter.com/4WU909Fjox
— Kambis Mashayekhi (@KambisMashayek1) May 30, 2024
Authors





1 comment
No intracoronary imaging????