Complicated subendothelial dissection during left anterior descending coronary artery – first diagonal branch bifurcation treatment with Culotte technique
Supported by the EuroIntervention Journal
Learn more about troubleshooting and tailor-made treatment combining 2D and 3D OCT thanks to this image in cardiology!
Authors
Michele Schincariol1*, Jiayue Huang2,3*, Harald Rittger1, Stylianos A. Pyxaras1, Shengxian Tu2
*Both authors contributed equally to the manuscript.
Case summary
An 84-year-old female patient with severe left anterior descending (LAD) – first diagonal (D1) bifurcation lesion (Medina classification 1,1,1) (Figure 1, Panel A) was electively treated with percutaneous coronary intervention (PCI) using the conventional Culotte technique (two-stent strategy), implanting the first stent into the most angulated branch (D1)1-3.
The LAD stent was a 2.5/28 mm drug eluting stent (DES) and it was extended longer into the proximal segment of the main vessel, whereas the D1 stent was a 2.5/22 mm DES.
Angiography performed after stent implantation revealed a filling-defect of the D1 stented segment (Figure 1, Panel A).
Multiple balloon dilatations, as well as thrombus aspiration, did not improve the angiographic phenotype.
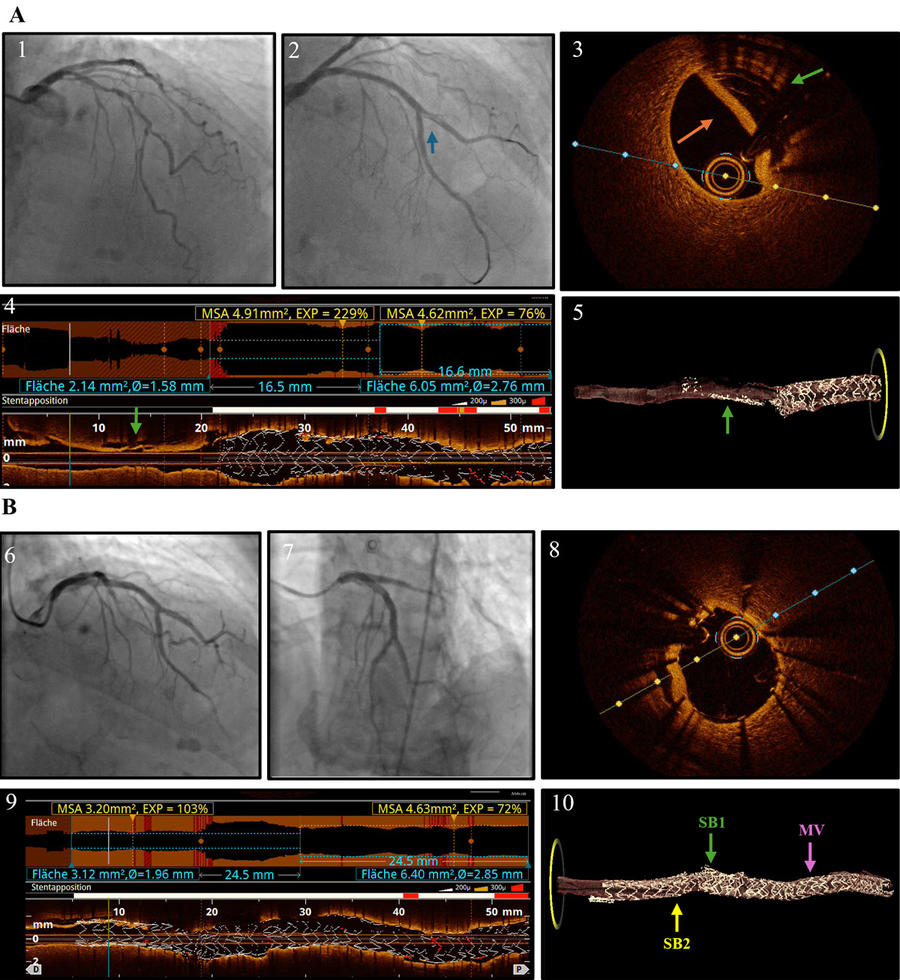
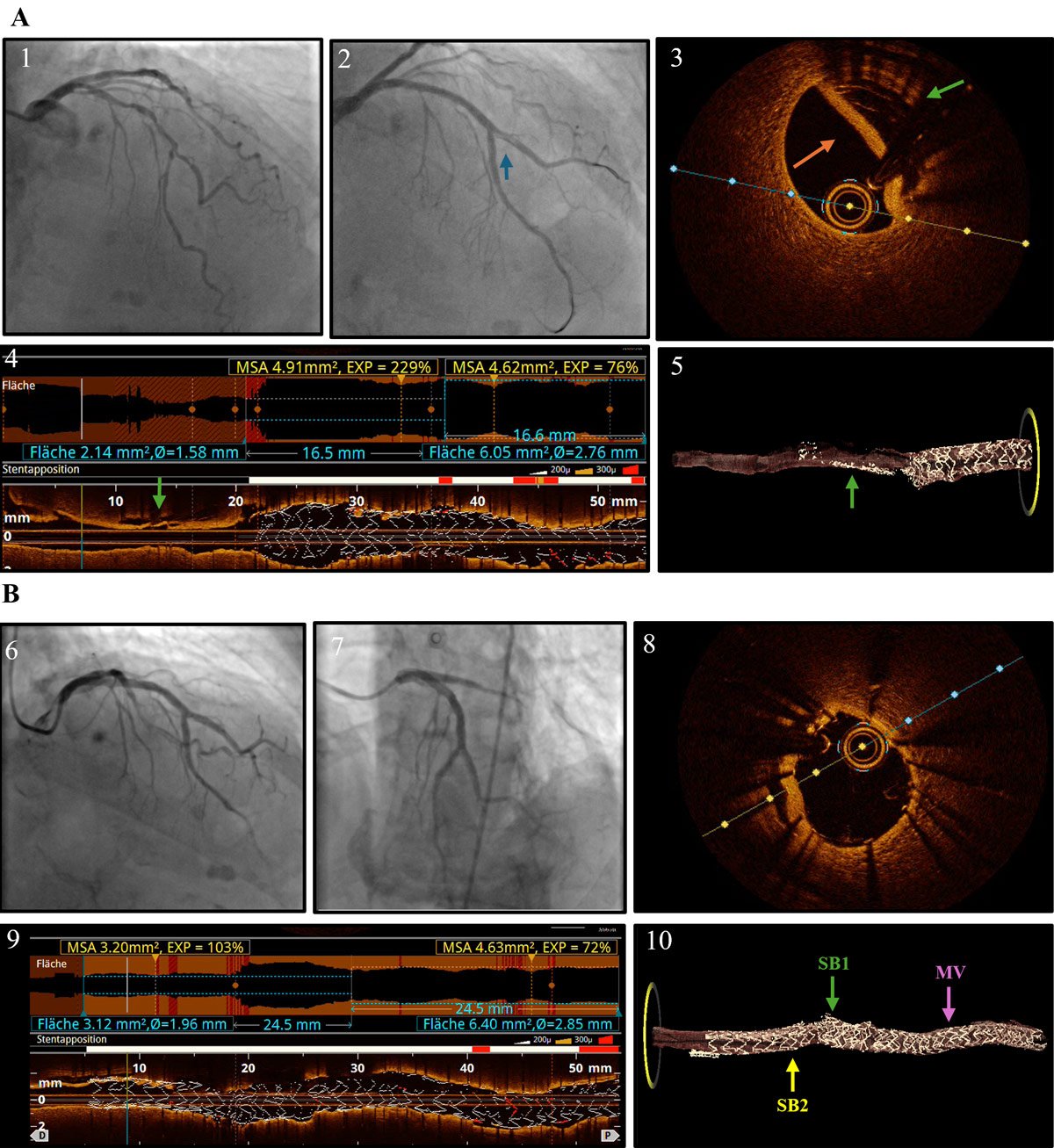
Figure 1. Troubleshooting of a complicated subendothelial dissection using 2D and 3D OCT.
- A) Angiography showing LAD/D1 bifurcation lesion (1); filling defect after stenting of D1 (blue arrow) (2); 2D OCT cross section displaying edge-stent dissection of D1 (orange arrow) and crushed stent within the sub-intimal space (green arrow) (3); 2D OCT longitudinal section displaying crushed stent within the sub-intimal space (green arrow) (4); 3D OCT reconstruction of partially crushed stent (green arrow) (5).
- B) Angiographic result after stenting of D1 (6,7); 2D OCT cross section displaying good stent expansion and exclusion of the dissection plane (8); 2D OCT longitudinal section showing exclusion of the dissection plane (9); 3D OCT reconstruction of the stent-in-stent implantation (10).
Optical coherence tomography (OCT) with three-dimensional (3D) reconstruction using a dedicated software (OctPlus software, Pulse Medical, Shanghai, China) revealed a distal edge-stent dissection of D1 and, proximally, a partially crushed stent within the sub-intimal space (Figure 1, Panel A and Video 1).
The presumed mechanism of stent crush might have been abluminal wiring of the previously implanted stent in D1 due to the omission of proximal optimization technique (POT). Guidance with OCT during the first procedure could have prevented this complication, as suggested by the results of the OCTOBER trial4.
Based upon the OCT-findings, a second stent (in-stent) was implanted in D1, connecting the proximal main-branch (MB) true-lumen to the D1 true lumen in a culotte-fashion (Figure 1, Panel B).
Good stent expansion and exclusion of the dissection plane were confirmed with both 2D and 3D-OCT (Figure 1, Panel B, and Video 2).
In this procedure, 3D-OCT-reconstruction was instrumental to allow precise diagnostic assessment of the stent-failure mode and, subsequently, tailor percutaneous coronary intervention.
Supplementary material
References
- Erglis A, Lassen JF, Di Mario C. Technical aspects of the culotte technique. EuroIntervention. 2015;11 Suppl V:V99-101.
- Chang CF, Chang KH, Lai CH, Lin TH, Liu TJ, Lee WL, Su CS. Clinical outcomes of coronary artery bifurcation disease patients underwent Culotte two-stent technique: a single center experience. BMC Cardiovasc Disord. 2019 Sep 2;19(1):208. doi: 10.1186/s12872-019-1192-2. PMID: 31477022; PMCID: PMC6719358.
- Lassen JF, Albiero R, Johnson TW, Burzotta F, Lefèvre T, Iles TL, Pan M, Banning AP, Chatzizisis YS, Ferenc M, Dzavik V, Milasinovic D, Darremont O, Hildick-Smith D, Louvard Y, Stankovic G. Treatment of coronary bifurcation lesions, part II: implanting two stents. The 16th expert consensus document of the European Bifurcation Club. EuroIntervention. 2022 Aug 19;18(6):457-470. doi: 10.4244/EIJ-D-22-00166. PMID: 35570753; PMCID: PMC11064682.
- Holm NR, Andreasen LN, Neghabat O, Laanmets P, Kumsars I, Bennett J, Olsen NT, Odenstedt J, Hoffmann P, Dens J, Chowdhary S, O'Kane P, Bülow Rasmussen SH, Heigert M, Havndrup O, Van Kuijk JP, Biscaglia S, Mogensen LJH, Henareh L, Burzotta F, H Eek C, Mylotte D, Llinas MS, Koltowski L, Knaapen P, Calic S, Witt N, Santos-Pardo I, Watkins S, Lønborg J, Kristensen AT, Jensen LO, Calais F, Cockburn J, McNeice A, Kajander OA, Heestermans T, Kische S, Eftekhari A, Spratt JC, Christiansen EH; OCTOBER Trial Group. OCT or Angiography Guidance for PCI in Complex Bifurcation Lesions. N Engl J Med. 2023 Oct 19;389(16):1477-1487. doi: 10.1056/NEJMoa2307770. Epub 2023 Aug 27. PMID: 37634149.
Affiliations
- Medizinische Klinik I, Klinikum Fürth, Academic Teaching Hospital of the Friedrich-Alexander-University Erlangen- Nürnberg, Fürth, Germany
- Biomedical Instrument Institute, School of Biomedical Engineering, Shanghai Jiao Tong University, Shanghai 200240, China
- The Lambe Institute for Translational Medicine, the Smart Sensors Laboratory and Curam, University of Galway, Galway, Ireland.
Conflicts of interest
- Prof. Tu is the cofounder of, has received research grants from, and been a consultant for Pulse Medical.
- Prof. Rittger reports consulting fees for Siemens and Speaker´s fees for Novartis, Pfizer, Astra and Boehringer.
- Dr. Pyxaras reports proctorship and consultancy fees from Asahi Intecc, Biotronik and Boston Scientific.
- Dr. Schincariol and Dr. Huang have no conflicts of interest to disclose.

No comments yet!