Percutaneous aspiration of vegetation to relieve obstruction in surgically repaired mitral valve
Supported by the EuroIntervention Journal
This image highlights the challenges of managing infective endocarditis (IE) and explores the potential role of transcatheter extraction devices in addressing unmet needs for patients who cannot undergo surgery.
Authors
Mohammad AlTermanini1, Hakam AlZaeem1, Mohammed AL-Hijji1
Introduction
Despite advancements in diagnostic and treatment techniques, infective endocarditis (IE) is associated with high rates of in-hospital death, ranging from 14 % to 24 %1. Due to concomitant illnesses, population aging, and greater use of prosthetic materials such as indwelling catheters and prosthetic valves, about 50 % of IE patients do not undergo indicated surgical intervention in the real-world experience2. Therefore, there is a large need for advancements in IE therapy. Recent small studies have shown the potential role of transcatheter extraction devices for the management of IE3-4.
Case summary
A 47-year-old man had a past medical history of hypertension, mitral valve prolapse, and a previous episode of infective endocarditis (IE) due to intravenous drug use, for which he underwent mitral valve repair using the Alfieri stitch with placement of a 3D memo Sorin annuloplasty ring in 2006.
He presented with fever and 3-day chills in the setting of likely relapse to intravascular drug use. Transthoracic echocardiography (TTE) revealed a large mobile mass of 1.2 x 2.5 cm attached to the atrial side of the mitral valve, leading to significant mitral valve stenosis, with a mean gradient across the mitral valve of 20 mmHg (Video 1).
Blood culture grew gram-positive cocci (Rothia mucilaginosa), and the diagnosis of infectious endocarditis (IE) was made. Based on the Heart Team discussion, surgery was declined as the risk for redo was very high, with also concern for recurrent prosthesis infection if he underwent valve replacement; therefore, an off-label percutaneous approach was chosen, using the 23-Fr 180-degree AngioVac system (AngioDynamics).
First, cerebral protection of any potential embolisation via a sentinel device (Boston Scientific) was performed prophylactically, due to the considerable risk of detachment of vegetation or its fragments during aspiration (Video 2).
Afterwards, a transseptal puncture at the posterior and middle parts of the fossa ovals was performed, and then the septum was dilated, using a 14 mm semi-compliant balloon to facilitate the delivery of AngioVac cannula across the septum through right femoral vein access.
The 15-Fr return cannula was positioned in the left femoral artery. After the funnel tip of the cannula was aligned with the mitral valve, the vegetation was successfully removed, using a 3-4 L/min flow (Figure 1) (Video 3).
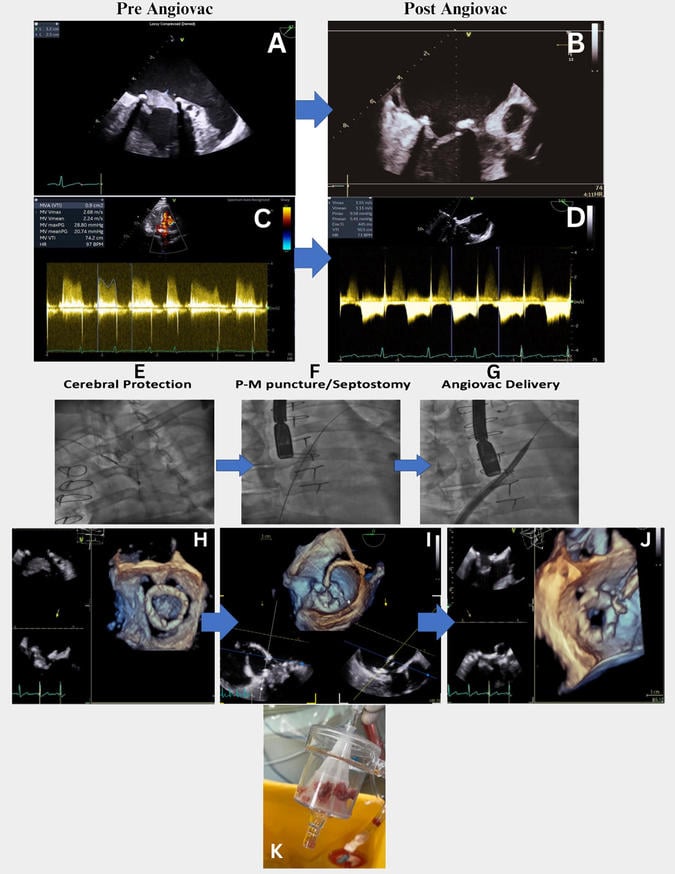
Figure 1: Percutaneous mechanical aspiration of vegetation adhered to repaired mitral valve with Alfieri stitch and ring annuloplasty using Angiovac system. A) Transesophagealechocardiogram (TEE) image revealedvegetation measuring (1.2cm x 2.5cm) on the atrial surface of the mitral valve causing complete obstruction of the mitral valve. B) TEE imageafter vegetation aspiration using the Angiovac system demonstrating successfully removedvegetation. C) Before aspiration of vegetation continuous wave (CW)doppler across mitral valve showing severe stenosis with a mean gradient across the mitral valve of 20 mmHg. D) Post-Angiovac aspiration CW doppler showing a significant decrease in mitral valve gradient to 5 mmHg. E) Prophylactic cerebral protection was performed using sentinel device. F) Trans-septal puncture at the posterior and middle part of the fossa ovals. G) Dilatation of septum using a semi-compliant balloon to facilitate delivery of AngioVac cannula. H) Pre-Angiovac aspiration of vegetation transesophageal Echocardiography (TEE) image using 3D Multiplanar Reconstruction (MPR) showing vegetation completely obliterating mitral valve. I) TEE MPR image showing engagement of Angiovac funnel tip with the vegetation before its removal with 1-2L/min flow,increased to 3.5–4 L/min flow while approaching the mitral valve mass for a total duration of 1-2mins. J) TEE MPR imagepost-Angiovac aspiration of vegetation demonstrating successfully removed vegetation and widely open mitral valve leaflets. K) Aspirated vegetation after Angiovac removal with culture revealed gram-positive cocci (Rothia mucilaginosa).
There was an immediate, significant decrease in gradient from 20 mmHg to 5 mmHg without complications (Video 4). The 26-Fr vein access was closed with the figure of 8 stitches and arterial with Proglide (Abbott) sutures.
The patient continued a 6-week antibiotic course, and he continued to do well at 8-month follow-up.
He underwent follow-up transthoracic echocardiography after 8 months, showing stable mitral valve function (mean gradient 5 mmHg) with no residual vegetation.
Conclusion
This case illustrates that the off-label use of percutaneous mechanical aspiration has a potential role in the management of infective endocarditis in patients who are at high risk or not suitable for surgical intervention. This approach is not risk-free as it can lead to some potential complications including bleeding, transient hemodynamic instability if air enters the circuit, and mass embolisation. These risks can be mitigated by careful pre-procedural planning, engaging the circuit before approaching the mass, and utilising cerebral protection device.
Supplementary material
References
- Olmos, C., Vilacosta, I., Fernández-Pérez, C. et al. The Evolving Nature of Infective Endocarditis in Spain: A Population-Based Study (2003 to 2014). JACC. 2017 Dec; 70(22): 2795–2804.
- Cahill TJ, Prendergast BD. Infective endocarditis. Lancet. 2016;387:882-89
- Xiao D, Dalton R, Fineman A, Benz M, Tsompanidis A. The use of AngioVac in a patient with severe infective endocarditis where open heart surgery is contraindicated: A case report. Cureus. 2023;15:e39639.
- Fiocco A, Colli A, Besola L. Case report: Treatment of left-sided valve endocarditis using the transapical AngioVac system and cerebral embolism protection device: A case series. Front Cardiovasc Med. 2023;10:1121488.
Affiliations
- Cardiology Department, Heart Hospital, Hamad Medical Corporation, Doha, Qatar
Conflicts of interest
All authors have been contributed in this study and declare no conflicts of interest related to the manuscript content.
No comments yet!