14 Apr 2026
Rapid CT-guided emergency TAVI-in-TAVI-in-valve for cardiogenic shock with high coronary obstruction risk
Supported by the EuroIntervention Journal
An 85-year-old man presented in cardiogenic shock with torrential aortic regurgitation after prior surgical and TAVI valve-in-valve procedures. With high coronary obstruction risk, urgent CT assessment and in-silico simulations guided a rapid redo TAVI-in-TAVI-in-valve implantation, demonstrating that CT-assisted emergency redo-TAVI is feasible and lifesaving in high-risk anatomies.
Authors
Dario Bongiovanni¹, Eva Harmel¹, Benedetta Grossi²³⁴, Damyan Penev¹, Korbinian Rothenaicher¹, Sebastien Elvinger¹, Letizia Maria Perri⁴, Giulia Luraghi⁴ and Philip W.J. Raake¹
- Department of Internal Medicine I, Faculty of Medicine, University Hospital of Augsburg, University Augsburg, Germany
- IRCCS Humanitas Research Hospital, Via Alessandro Manzoni 56, 20089 Rozzano, Milan, Italy.
- Department of Biomedical Sciences, Humanitas University, Milan, Italy
- Department of Chemistry, Materials and Chemical Engineering, Politecnico di Milano, Milan, Italy.
Acute presentation: cardiogenic shock and severe aortic regurgitation
An 85-year-old man presented to the emergency department with acute dyspnea and chest pain.
Chest X-ray showed pulmonary oedema; echocardiography revealed torrential aortic regurgitation, and high-sensitivity troponin T was elevated (1,200 pg/ml; normal < 14 pg/ml).
The patient had undergone surgical aortic valve replacement (25 mm Perimount bioprosthesis) in 2010, followed by valve-in-valve TAVI with a self-expanding device (29 mm Evolut) in 2020.
Urgent coronary angiography was performed for suspected acute coronary syndrome. Selective intubation of both coronary ostia was challenging, owing to the TAVI prosthesis.
The right coronary artery (RCA) was assessed by non-selective aortic root angiography (Figure 1A).
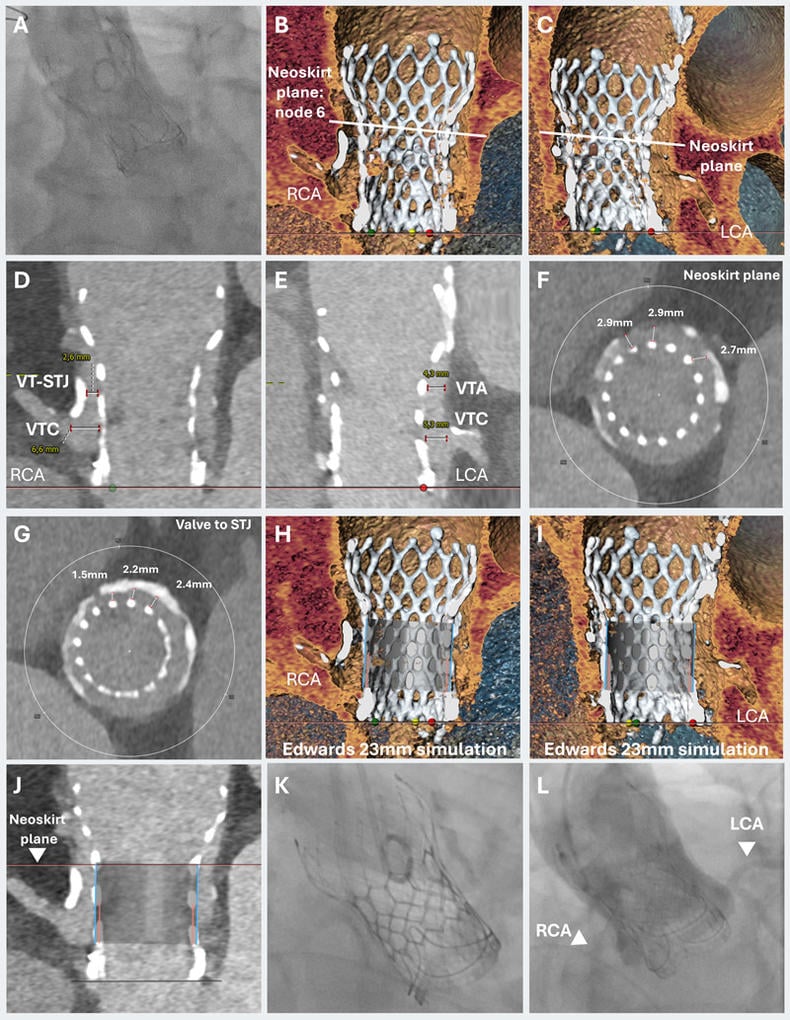
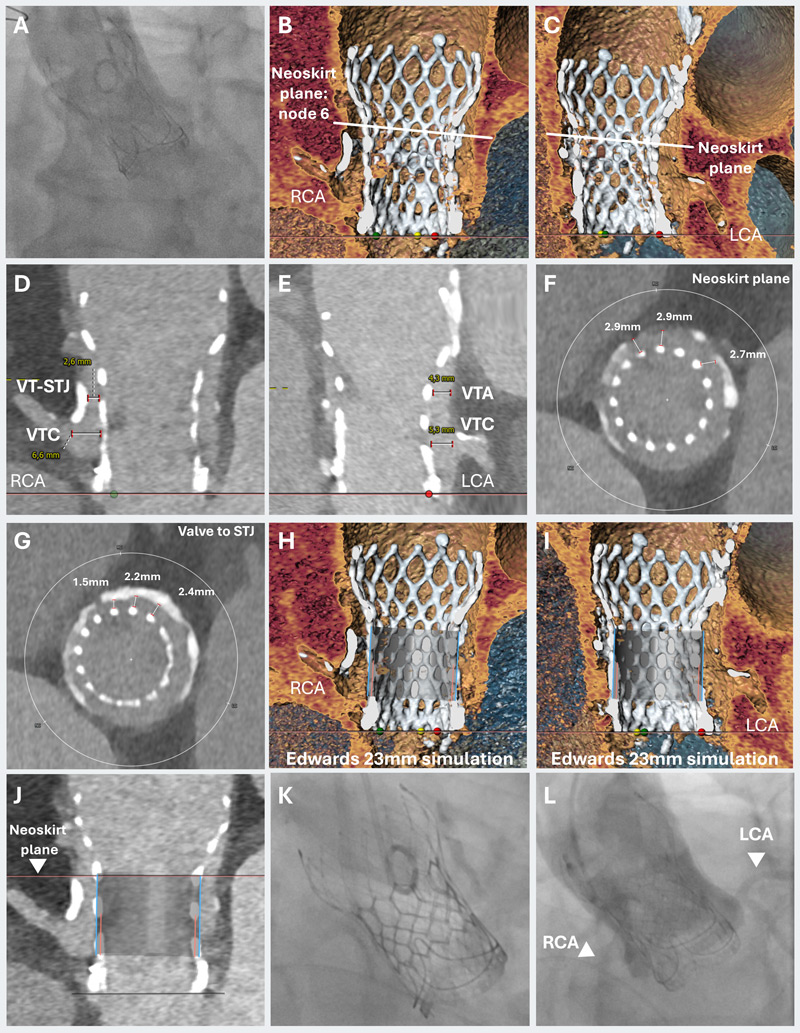
Figure 1: TAVI-in-TAVI-in-valve for cardiogenic shock with high coronary obstruction risk.
A) Non-selective aortic root angiography of the right coronary artery.
B-C) CT-analysis with virtual valve simulation defined the neoskirt plane.
D-G) The valve-to-coronary (VTC) distance measured 6.6 mm for the right coronary artery (RCA) and 5.3 mm for the left coronary artery (LCA), while valve-to-sinotubular junction (VT-STJ) distance ranged from 1.5 to 2.6 mm for the right cusp and exceeded 4 mm for the left cusp.
H-J) These findings indicated a high risk of RCA obstruction but preserved feasibility for redo implantation with targeted positioning at node 6 to the Evolut valve.
K-L) Final valve position showing stable seating without residual aortic regurgitation. Aortography confirmed preserved and unobstructed perfusion of both coronary arteries.
The aortic pressure curve was ventricularised, confirming torrential aortic regurgitation.
The patient deteriorated into cardiogenic shock, and emergency redo-TAVI was planned (Moving image 1).
CT assessment and coronary obstruction risk
Despite haemodynamic instability, CT was obtained under non-invasive ventilation. CT analysis with virtual valve simulation delineated the neoskirt plane (Figures 1B and 1C) and a VIVID type IIIB-like risk profile for coronary obstruction: valve-to-coronary (VTC) distance 6.6 mm (RCA) and 5.3 mm for the left coronary artery (LCA); valve-to-sinotubular junction (VT–STJ) ranged from 1.5 to 2.6 mm for the right cusp and > 4 mm for the left cusp (Figures 1D to 1G).
These findings indicated high risk of RCA obstruction, yet feasibility for redo implantation with targeted positioning at node 6 of the Evolut valve (Figures 1H to 1J).
In-silico simulation of the procedure confirmed feasibility, highlighting neoskirt formation during valve deployment (Moving Image 2).
CT-guided redo-TAVI without contrast
The patient was intubated and transferred directly to the catheterisation laboratory. Via single right femoral arterial access, a 23-mm Edwards SAPIEN 3 Ultra valve was implanted with no contrast dye injection, guided by CT-informed fluoroscopy and planning (Moving image 3).
The valve was well seated, without residual aortic regurgitation. Aortography confirmed unobstructed perfusion of both coronary arteries (Figures 1K and 1L; Moving image 4). The patient was transferred to intensive care on vasopressors, improved hemodynamically, and was extubated the following day.
Emergency redo-TAVI: key take-home messages
Redo-TAVI carries a heightened risk of coronary occlusion1. Nevertheless, the need for redo-TAVI is rising as TAVI is increasingly performed in younger patients who are more likely to outlive their index bioprosthesis.
Although no universally accepted, cut-offs exists for VT–STJ or VTC, a VTC < 4 mm is consistently associated with a high risk of coronary obstruction, and a VT–STJ < 3.5 mm is likewise considered high-risk2.
To our knowledge, this is the first reported case of emergency valve-in-valve redo TAVI (TAVI-in-TAVI-in-valve) in a patient at high risk for coronary obstruction (VT-STJ 1.5-2.6 mm), successfully performed within four hours from angiography to implantation.
Rapid CT assessment of VTC, VT–STJ, and VTA parameters was decisive for treatment guidance.
Emergent TAVI can be lifesaving in cardiogenic shock3,4, but redo procedures require meticulous CT evaluation and precise implantation planning.
This case demonstrates that CT-assisted emergency redo-TAVI is feasible, and that careful CT analysis, complemented by in-silico simulations, can enable treatment even in high-risk anatomies, such as VIVID type III.
Conflict of interest statement
The authors declare that they have no conflicts of interest.


1 comment
IMPRESSIVE CASE. THE SHORT DURATION OF THE TAV IN SAV IS NOTABLE. IT WOULD BE INTERESTING TO KNOW IF THE EVOLUT VALVE WAS POST-DILATED, WHICH COULD CONTRIBUTE TO ITS DETERIORATION.