Sex-specific outcomes after transcatheter or surgical treatment of aortic valve stenosis: the DEDICATE-DZHK6 trial
Selected in European Heart Journal by R. Sava
Women have long been underrepresented in TAVR trials. This article explores the DEDICATE trial’s sex-specific outcomes after TAVI and SAVR, revealing differences in early stroke risk, procedural challenges, and one-year survival in men and women with aortic stenosis.
References
Authors
Sabine Bleiziffer, Florian Leuschner, Tanja K Rudolph, Reinhard Vonthein, Anna L Meyer, Karl Georg Haeusler, Ulrich Hofmann, Armin Gorski, Andreas Hagendorff, Won-Keun Kim, Helmut Baumgartner, Michael A Borger, Yeong-Hoon Choi, Jochen Cremer, Volkmar Falk, Norbert Frey, Christian Hagl, Inke R König, Ulf Landmesser, Steffen Massberg, Hermann Reichenspurner, Matthias Renker, Holger Thiele, Thomas Walther, Andreas Ziegler, Stefan Blankenberg, Henryk Dreger, Rawa Arif, Axel Unbehaun, Moritz Seiffert, for the DEDICATE Study Investigators
Reference
European Heart Journal, Volume 47, Issue 11, 14 March 2026, Pages 1339–1353
Published
14 March 2026
Link
Read the abstractReviewer

My Comment
DEDICATE TAVR vs SAVR: sex specfic outcomes - proposed by Ruxandra Sava for PCRonline
Why this study – the rationale/objective?
Women have consistently been underrepresented in randomised transcatheter aortic valve replacement (TAVR) trials, despite aortic stenosis (AS) occurring with similar frequency in women and men. The DEDICATE-DZHK6 trial1, designed to reflect real-world practice, allowed an unrestricted choice of TAVR devices and enrolled 44% women.
This pre-specified subgroup analysis aimed to address this gap in knowledge by evaluating sex-specific peri-procedural characteristics and outcomes in low- to intermediate-risk patients undergoing TAVI or surgical aortic valve replacement (SAVR).
How was it executed – the methodology?
DEDICATE2 was an investigator-initiated, multicentre, 1:1 randomised controlled study comparing outcomes after TAVR and SAVR for the treatment of severe, symptomatic AS in patients with a Society of Thoracic Surgeons predicted risk of mortality (STS-PROM) < 4%, at 38 German study centres.
Patients aged 65-85 years old could be included in the trial. Bicuspid AS was excluded.
The primary outcome (PO) was the composite of all-cause death or stroke at one and five years. To exclude the influence of relevant confounders such as annulus area, STS-PROM score and trial site, a multiple Cox regression analysis was performed.
What is the main result?
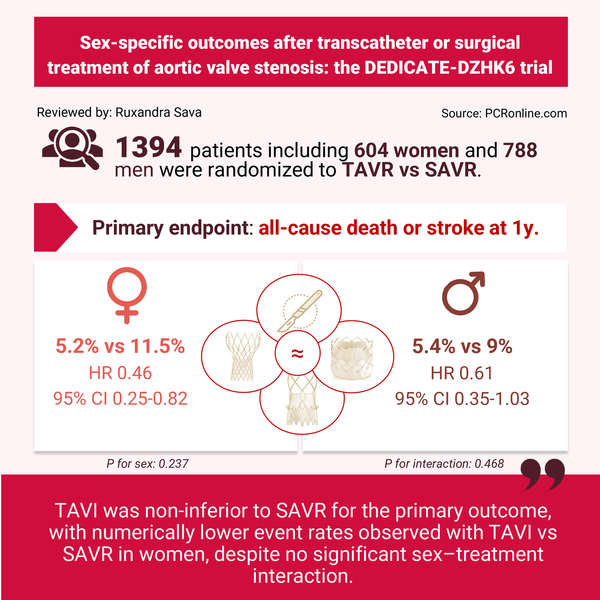
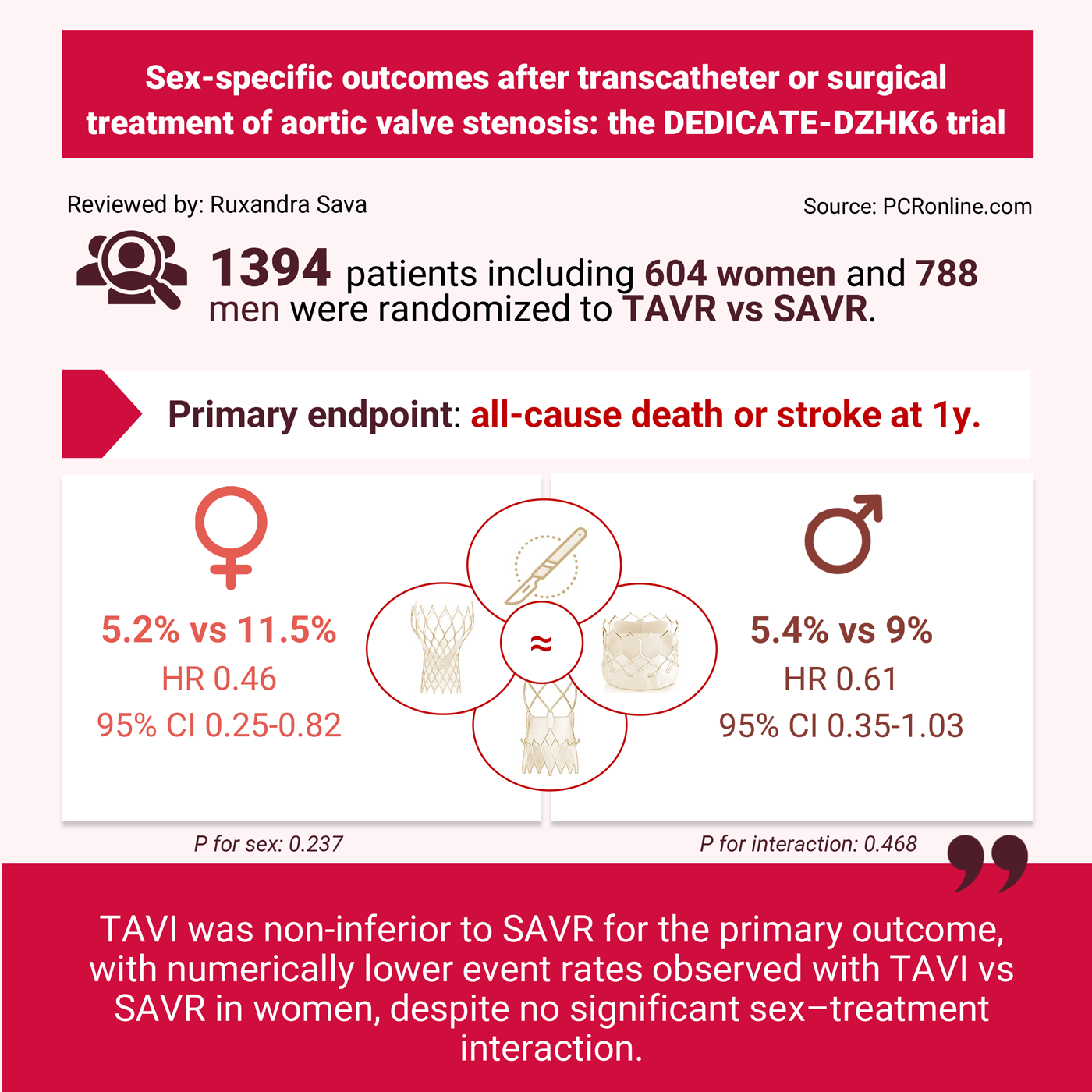
Sex-specific data was available for 1,394 patients, out of which 604 were women and 788 were men. By comparison to men, women were predicted to be at higher risk (median STS-PROM 2.1% vs 1.5%, P < 0.001) and more often presented with NYHA class 3 or higher (51% vs 42%, P <0.001). As expected, women had smaller aortic annuli and common femoral artery dimensions.
Men, however, had a higher burden of comorbidity, with greater prevalence of diabetes mellitus, coronary artery and peripheral vascular disease, chronic obstructive pulmonary disease, and atrial fibrillation.
The primary outcome of all-cause death or stroke:
- At 30-days: women had higher rates of the PO than men after both TAVR and SAVR, with no significant sex-treatment interaction (TAVR: 3.6% vs 1.5%, HR 0.63, 95% CI 0.29-1.32; SAVR: 5.8% vs 2.5%, HR 0.65, 95% CI 0.23-1.7, P for sex = 0.036).
- At one year: there was no significant interaction between sex and treatment (P = 0.468), and no significant difference between women and men was observed (P = 0.237). However, in women TAVR was associated with a significantly lower rate of the PO compared with SAVR (5.2% vs 11.5%, HR 0.46, 95% CI 0.25–0.82), whereas in men there was no statistically significant difference (5.4% vs 9%, HR 0.61, 95% CI 0.35–1.03).
Critical reading and the relevance for clinical practice:
This sub-analysis of the DEDICATE trial demonstrated that by comparison to men, women had an early excess risk of the primary composite outcome of all-cause death and stroke, primarily driven stroke. At 30 days, among women, the risk of stroke after SAVR was twice that seen after TAVR. At one year, although the overall sex difference was no longer apparent, among women, SAVR remained associated with higher rates of stroke (HR 0.43, 95% CI 0.18–0.93) and disabling stroke (HR 0.18, 95% CI 0.03–0.59) compared with TAVR, without evidence of a significant sex–treatment interaction.
Several important limitations should be considered when interpreting this data: this was a purely exploratory analysis that was not powered for statistical significance, overall event rates were low and no adjustments were made for multiple testing.
By comparison, in the RHEIA trial3, which enrolled predominantly low-risk women (median STS-PROM 2%) and randomised them to TAVR with a balloon-expandable valve or SAVR, stroke rates were similarly low regardless of treatment strategy. However, TAVR was associated with lower rates of the primary outcome of all-cause death, stroke, or rehospitalisation.
In the SURTAVI trial4, which randomised intermediate risk patients (median STS PROM of 4.5%) to TAVR with a supra-annular valve or SAVR, stroke rates were significantly higher with SAVR than with TAVR in men, but not in women. While women suffered from more TAVR procedural complications than men, survival was not impacted. Finally, TAVR was associated with more rapid functional capacity in both sexes, with women showing a greater magnitude of improvement at 30 days and one year.
The present study addresses the interaction between annular size and hemodynamics in men and women. Despite woman having smaller annuli than men, aortic valve mean gradients and area at discharge and at one year were similar to men’s, regardless of treatment allocation. Interestingly, a supra-annular valve such as Accurate or Evolut was chosen for a larger proportion of women than of men treated by TAVI (40.3 vs 22.9%). In the SAVR cohort, sutureless valves were more often used in women; data regarding the use of root-enlargement strategies was not reported. These results are consistent with the SURTAVI trial, in which TAVR with supra-annular valves was associated with lower mean gradients and similar rates of prosthetic-patient mismatch between men and women4. Overall, these findings suggest that adequate selection of contemporary strategies can lead to favorable hemodynamics regardless of annular size.
Another interesting procedural finding was that women more often required valve post-dilation than men (31% vs 17.4%, p < 0.001). However, pre-dilation was performed numerically less often in women (46.2% vs 51.3%, p = 0.182). This may be partly explained by the fact that women present with less aortic valve calcifications, but with increased fibrosis. As the latter cannot be reliably detected pre-procedurally, the requirement for valve pre-dilation may indeed be underestimated in women, leading to a higher requirement of post-dilatation due to residual transvalvular gradients. Furthermore, predominance of fibrosis over calcification may also be associated with less favorable anchoring for a TAVR prosthesis, and all six events of prosthesis malposition or embolization occurred in women.
Overall, this study adds to the evidence that TAVI is non-inferior to SAVR at one year, with numerically lower rates of death and stroke in women. Given the consistent observation of higher early complication rates in women following aortic valve replacement, treatment decisions between TAVR and SAVR should carefully consider the severity of presentation, functional status, frailty, comorbidities, and patient preferences.
References
- Surgical treatment of aortic valve stenosis: the DEDICATE-DZHK6 trial. Eur Heart J. 2026;47(11):1339-1353. doi:10.1093/eurheartj/ehaf519
- Seiffert M, Vonthein R, Baumgartner H, et al. Transcatheter aortic valve implantation versus surgical aortic valve replacement in patients at low to intermediate surgical risk: rationale and design of the randomised DEDICATE Trial. doi:10.4244/EIJ-D-23-00232
- Tchetche D, Pibarot P, Bax JJ, et al. Transcatheter vs. surgical aortic valve replacement in women: the RHEIA trial. Eur Heart J. 2025;46(22):2079-2088. doi:10.1093/eurheartj/ehaf133
- Mieghem NMV, Reardon MJ, Yakubov S, et al. Clinical outcomes of TAVI or SAVR in men and women with aortic stenosis at intermediate operative risk: a post hoc analysis of the randomised SURTAVI trial. doi:10.4244/EIJ-D-20-00303


No comments yet!