29 Jan 2021
The Controlled Antegrade and Antegrade Tracking (CAAT) technique for left main trunk bifurcation divided by a flap-like structure
Supported by the EuroIntervention Journal
The authors present a case of PCI for left main trunk bifurcation divided by a flap-like structure in a 67-year-old man suffering from effort angina, in which they successfully used a novel tracking technique by modifying the reverse controlled antegrade and retrograde tracking (CART), which they called the controlled antegrade and antegrade tracking (CAAT) technique.
Authors
Masanobu Ishii1, Kazumasa Kurogi1, Nobuyasu Yamamoto1, Kenichi Tsujita2
Case summary
We present a case of percutaneous coronary intervention for left main trunk (LMT) bifurcation divided by a flap-like structure in a 67-year-old man suffering from effort angina, in which we successfully used a novel tracking technique by modifying the reverse controlled antegrade and retrograde tracking (CART)1, which we called the controlled antegrade and antegrade tracking (CAAT) technique.
Coronary angiography showed a filling defect in LMT bifurcation (Figure A-A’ and Video 1-2).
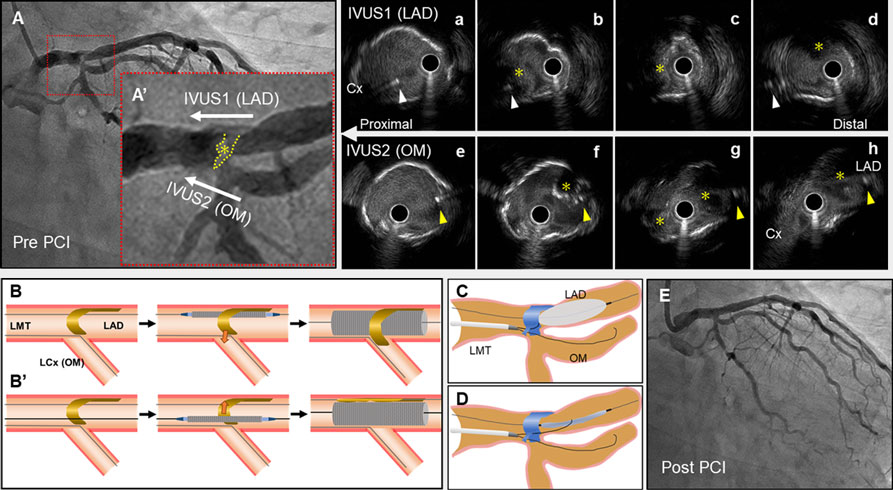
(A, A’) Angiography of left coronary artery before PCI.
(a-d) Intravascular ultrasound (IVUS) image from left anterior descending artery (LAD) to left main trunk (LMT), (e-h) IVUS image from obtuse marginal branch (OM) of left circumflex to LMT, (a, e) LMT level, (b, c, f, g) LMT bifurcation level, (d) LAD proximal level, (h) LCX ostium level.
White arrowhead indicates the guidewire of OM; yellow arrowhead, the guidewire of LAD; (*), the flap-like structure.
(B, B’) Schema of the LMT-LAD crossover stenting strategies without (B) and with (B’) the controlled antegrade and antegrade tracking technique.
(C, D) Schema of the controlled antegrade and antegrade tracking technique.
(E) Final angiographic result.
The image of intravascular ultrasound (IVUS) pullback from the left anterior descending artery (LAD) to LMT (Figure a-d) revealed that the flap-like structure laid in a spiral from 12 o’clock to 9 o’clock, and the structure occluded the distal of left circumflex (LCX) ostium. In addition, the image of IVUS from obtuse marginal branch (OM) of LCX (Figure e-h) revealed that the structure seemed to be floating at the LCX ostium. Those findings suggested that the structure would have easily caused occlusion of LCX ostium if cross-over stenting from LAD to LMT had been performed (Figure B).
The floating structure remained after several attempts of an excimer laser coronary atherectomy for plaque volume reduction by its tissue ablation mechanism. Next, in order to push the flap-like structure away from LCX ostium after stenting (Figure B’), we advanced the Gaia Next 2 (Asahi Intecc Co., Ltd, Japan) to avoid the flap-like structure using a double lumen catheter, SASUKE (Asahi Intecc Co., Ltd, Japan), on the guidewire of OM, resulting in subintimal tracking of LAD.
Therefore, we advanced the Gaia next 2 towards the inflated balloon of 3.0-mm located in LAD, for the reduction of subintimal space. With balloon deflation, the Gaia next 2 was successfully advanced into the proximal true lumen of LAD (Figure C-D and Video 3), avoiding the flap-like structure in the LMT bifurcation, subsequently followed by stenting from the LAD to LMT with a drug-eluting stent, showing an excellent final angiography without occlusion of LCX (Figure E and Video 4).
Similar techniques have been previously proposed to exclude foreign bodies from the vessel lumen, by burying them deep into the vessel wall, however, this is the first report proposing a technical name for the technique, that is the CAAT technique and proposing its use to prevent occlusion of side branches in the main bifurcation lesion without excessive expansion of subintimal hematoma and dissection.
Conflict of interest statement
Dr. Tsujita has received honoraria from Bayer Yakuhin, Ltd., Daiichi Sankyo Co., Ltd., Kowa Pharmaceutical Co. Ltd., MSD K.K., Sanofi K.K., and Takeda Pharmaceutical Co., Ltd.; has received trust research/joint research funds from AstraZeneca K.K., Sugi Bee Garden, and Japan Medical Device Technology Co., Ltd.; and has received grants from ITI Co., Ltd., Astellas Pharma Inc, Abbott Vascular Japan Co., Ltd., Otsuka Pharmaceutical Co., Ltd., Kaneka Medix Co., Ltd., Goodman Co., Ltd., GM Medical Co., Ltd., Daiichi Sankyo Co., Ltd., Takeda Pharmaceutical Co., Ltd., Mitsubishi Tanabe Pharma, Chugai Pharmaceutical Co., Ltd., TERUMO Co., Ltd., Boehringer Ingelheim Japan, Medtronic Japan Co., Ltd., Japan Lifeline Co., Ltd., Novartis Pharma K.K., Fides-One, Inc., Bristol-Myers K.K., Boston Scientific Japan K.K., Cardinal Health Japan, and MSD K.K. All the other authors have nothing to disclose.
Affiliations
- Department of Cardiovascular Center, Miyazaki Prefectural Nobeoka Hospital, Nobeoka, Japan.
- Department of Cardiovascular Medicine, Graduate School of Medical Science, Kumamoto University, Kumamoto, Japan.
References
- Matsuno S, Tsuchikane E, Harding SA, Wu EB, Kao HL, Brilakis ES, Mashayekhi K, Werner GS. Overview and proposed terminology for the reverse controlled antegrade and retrograde tracking (reverse CART) techniques. EuroIntervention 2018; 14: 94-101.

2 comments
The author has used two guide wires to prevent occlusion of healthy LCX ostium .I feel partially inflatted balloons one in LCX ostium and another one in OM1 ostium would have provided more protection against thrombus shifting
I partially agree with Barick, but only as a bailout procedure, for a LCX occlusion after placing the stent in LM and LAD.