Distal radial approach to reaccess and recanalize the occluded radial artery
Supported by the EuroIntervention Journal
A 56-year-old man was re-admitted with chest pain. He had been hospitalized 2 weeks before because of MI, was suffering from metastatic carcinoma with recurrent PTE, and was on long-term subcutaneous heparin...
Authors
Karthick Manoharan1, Pitt O Lim1
Case summary
A 56-year-old man was re-admitted with chest pain. He had been hospitalized 2 weeks before because of myocardial infarction (MI), was suffering from metastatic carcinoma with recurrent pulmonary thromboembolism (PTE), and was on long-term subcutaneous heparin.
Then, he had a 6Fr right radial artery (RA) coronary procedure. The mid-LAD was re-opened with balloons, restoring flow with residual adherent non-occlusive thrombus.
A repeat coronary angiography was performed. He had radial artery occlusion (RAO), as evidenced by loss of pulse and a negative reverse Allen’s test with pulse oximetry.
Despite this, the artery was accessed via the distal RA (dRA) using the 2-step cannulation technique we previously described1, initially with a pedal-access microcatheter (Cook Medical, Bloomington, IN, USA). Radial arteriogram (Figure 1A, Video 1) confirmed a thrombosed RA.
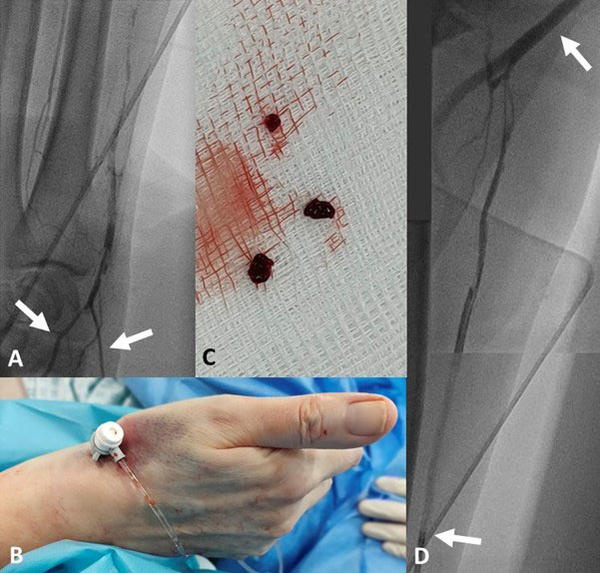
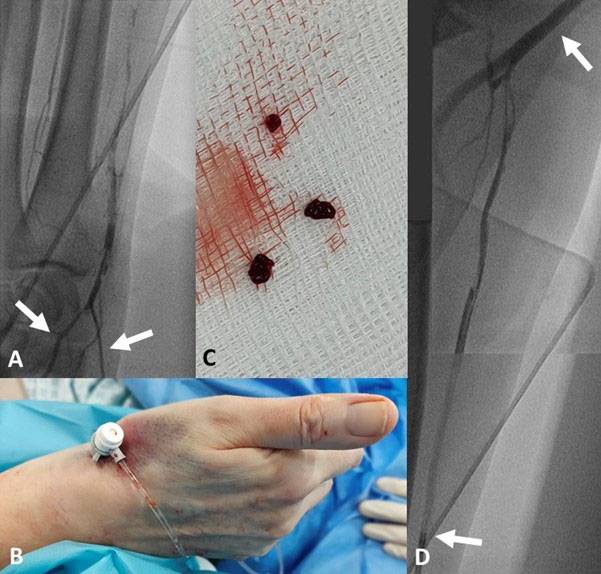
Figure 1
1A – Superficial palmar arch branch (left arrow) and Microcatheter (right arrow).
1B – dRA approach with a 5Fr “femoral” sheath.
1C – Aspirated thrombi.
1D – Recanalized RA with residual thrombi, tip of guide (lower arrow) and brachial artery (upper arrow).
Next, a 0.035” J-tipped wire, which is more supportive, was used to swap in a 5Fr “femoral” sheath (Figure 1B), and a 4Fr JR4 catheter was advanced to the RA ostium, aspirated and flushed, and heparin was given to avoid thromboembolization.
The RCA was imaged, and an EBU 3.5 5Fr guide was then used with similar safety caveats, which revealed a shrinking thrombus at the mid-LAD.
The guide was then withdrawn from the RA and aspiration thrombectomy performed (Figure 1C), with improved flow down the RA (Figure 1D, Video 2).
The Achilles’ heel of the RA access is RAO² and the dRA approach might well turn out to be its homing arrow³.
It offers natural patent haemostasis with continuation of flow into the hand via the superficial palmar arch branch when the access site is compressed following sheath removal.
In our case, arguably it is better to reuse the right RA than to risk bilateral RAO if the contralateral RA was used. It is also possible that the right RA would remain patent.
Furthermore, while the dRA approach is associated with less RAO, it does not reduce procedural prowess as offered by the RA access¹,⁴.
We predict that within the next 2 years, there will be sufficient data from randomized controlled trials to support its use as default radial access³.
Conflict of interest statement
The authors have no conflict of interest to declare.
References
- Ferreira-Martins, J. and P.O. Lim, Two-Step Distal Radial Artery Cannulation for Challenging Radial Anatomies. Cardiology, 2021. 146(2): p. 144-150.
- Bernat, I., et al., Best Practices for the Prevention of Radial Artery Occlusion After Transradial Diagnostic Angiography and Intervention: An International Consensus Paper. JACC Cardiovasc Interv, 2019. 12(22): p. 2235-2246.
- Eid-Lidt, G., et al., Distal Radial Artery Approach to Prevent Radial Artery Occlusion Trial. JACC Cardiovasc Interv, 2021. 14(4): p. 378-385.
- Manoharan, K. and P.O. Lim. (2021, March 17). Overcoming the 360 Degree Radial Artery Loop. Retrieved from https://www.pcronline.com/Cases-resources-images/Images-interventional-cardiology/EuroIntervention-images/Overcoming-the-360-degree-radial-artery-loop
Affiliation
- Department of Cardiology, St George’s Hospital, London, UK
No comments yet!