02 Mar 2021
Intercostal embolization of a stuck rotational atherectomy burr
Supported by the EuroIntervention Journal
An elective right coronary artery PCI was scheduled in an 83-year-old gentleman. Due to the presence of severely diffuse and calcified disease, rotational atherectomy was decided, but the burr got entrapped in the severely calcified and tortuous proximal segment of the artery...
Authors
Eduardo Arroyo-Úcar1,2, Gonzalo Pizarro Sánchez3-6, Raúl Moreno7, Francisco Torres-Saura1,2.
Case summary
Rotational atherectomy (RA) (Boston Scientific, Marlborough)-typically used in complex percutaneous coronary interventions (PCI) - modifies calcified lesions by using a diamond-encrusted burr that rotates at high speed (140,000 to 180,000 rpm)1. The stuck of the burr is a rare but life-threatening complication.
An elective right coronary artery PCI was scheduled in an 83-year-old gentleman. Due to the presence of severely diffuse and calcified disease, RA was decided (Figure 1A, video 1).
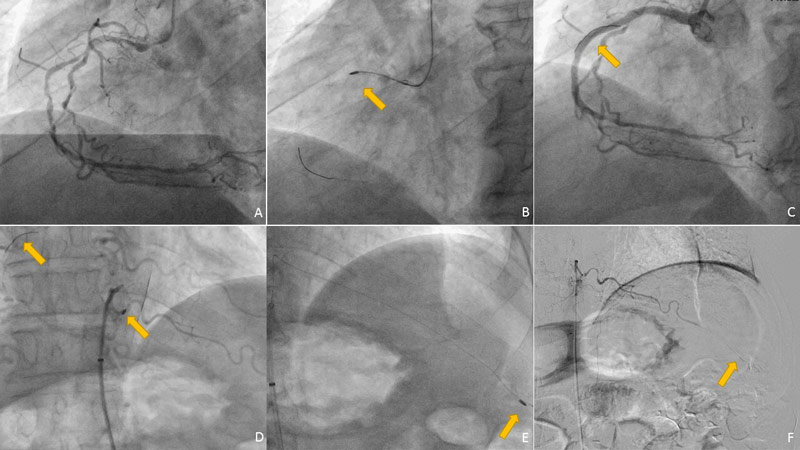
Figure 1 - 1A: Right coronary artery angiography, showing multisegment calcified lesions. 2A: 1,25 mm burr entrapped in the proximal right coronary artery. 3A: Final result after PCI in the right coronary artery, with the fragment of the RotaWire covered with a drug eluting stent. 4A: Selective angiography of the intercostal artery showing the embolizated burr. 5A: Mobilization of the burr after various attempts of recover (microcatheter). 6A: Final angiography with distal embolization of the burr and thrombosis of the artery.
The 1.25 mm burr (170,000 rpm) was suddenly entrapped in the severely calcified and tortuous proximal segment of the artery (Figure 1B, video 2).
The sheath was cut off and the outer cover of the Rotablator was removed, in order to use an extension catheter (EC). A second wire did not cross the lesion, and thus aggressive manual pullback was performed. RA catheter could be released, however RotaWire and inner cover broke, and consequently burr embolized to aorta. A shard of the RotaWire was left in the proximal right coronary artery, which could be finally covered with 4 everolimus-eluting stents with good results (Figure 1C, video 3). Abdominal aortography demonstrated intercostal-artery location of the burr (Figure 1D, video 4-5).
Selective canalization of this artery allowed 0,014´wire crossing, but recapture was not possible despite using different types of devices (micro-catheter, snare, thrombus aspiration catheter, Figure 1E, video 6-7). Burr was finally pulled distally, causing thrombosis and stabilization of the fragment (Figure 1F, video 8).
Patient could be discharged without significant postprocedural complications and did not develop any symptoms or biochemical manifestations of the intercostal artery occlusion.
General management of a stuck RA burr includes gradually2:
- Recross with a second wire, and inflate a balloon to try to mobilize the burr
- Deep intubation or use an EC to pull the burr inside the catheter
- Surgical removal of the burr
Usually, patients present hemodynamic instability, as a stuck burr can be occlusive and interrupt coronary flow. Given the complex coronary anatomy and the presence of calcium, percutaneous retrieval of a stuck burr is a challenging scenario.
Sulimov et al reported up to 38.9% of surgical removal3. Thus, aggressive attempts of pulling with deep intubation or using an EC are recommended, so traction force is applied to the burr. Ineffective traction can lead to inner cover rupture, remaining the entrapped burr inside the artery or as in our case generating aortic embolization. No previous cases have been reported.
This image should be kept in mind, as in any other complications, outcome could have been catastrophic4.
Conflict of interest statement
The authors do not have conflicts of interest
References
- Serra A, Jiménez M. Rotational atherectomy and the myth of Sisyphus. EuroIntervention J Eur Collab with Work Gr Interv Cardiol Eur Soc Cardiol. 2020;16(4):e269-e272. doi:10.4244/EIJV16I4A45
- Giannini F, Candilio L, Mitomo S, Ruparelia N, Chieffo A, Baldetti L, Ponticelli F, Latib A, Colombo A. A Practical Approach to the Management of Complications During Percutaneous Coronary Intervention. JACC Cardiovasc Interv. 2018;11(18):1797-1810. doi:10.1016/j.jcin.2018.05.052
- Sulimov DS, Abdel-Wahab M, Toelg R, Kassner G, Geist V, Richardt G. Stuck rotablator: the nightmare of rotational atherectomy. EuroIntervention J Eur Collab with Work Gr Interv Cardiol Eur Soc Cardiol. 2013;9(2):251-258. doi:10.4244/EIJV9I2A41
- Isogai T, Yasunaga H, Matsui H, Tanaka H, Fushimi K. Relationship between hospital volume and major cardiac complications of rotational atherectomy: A nationwide retrospective cohort study in Japan. J Cardiol. 2016;67(5):442-448. doi:10.1016/j.jjcc.2015.07.008
Affiliations
- Unidad de Cardiología Intervencionista, Hospital Universitario del Vinalopó, Elche, Alicante, Spain.
- Unidad de Cardiología Intervencionista, Hospital Universitario de Torrevieja, Alicante, Spain.
- Centro Nacional de Investigaciones Cardiovasculares Carlos III (CNIC), Madrid, Spain.
- Centro de Investigación Biomédica en Red de Enfermedades Cardiovasculares (CIBERCV), Madrid, Spain.
- Servicio de Cardiología, Complejo Hospitalario Ruber Juan Bravo, Madrid, Spain.
- Departamento de Cardiología, Facultad de Medicina, Universidad Europea de Madrid (UEM), Madrid, Spain.
- Unidad de Cardiología Intervencionista, Hospital Universitario La Paz, Madrid, Spain.


1 comment
Wonderful case!