17 Jul 2020
Swinging through the Web; Mitraclip implantation in a patient with giant Chiari Network
Supported by the EuroIntervention Journal
A 42-year-old man with primary MR secondary to P2 prolapse of the mitral valve (MV), presented with dyspnea on exertion...
Authors
Ganapathi Palaniappan1, Aslannif Roslan1, Mohd Nasir Muda1, Amin Ariff Bin Nuruddin1
Case summary
A 42-year-old man with primary mitral regurgitation secondary to P2 prolapse of the mitral valve (MV), presented with dyspnea on exertion. Transthoracic Echo (TTE) showed preserved LV function of 63%, thickened posterior mitral valve leaflet (PMVL) and ruptured P2 scallop chord resulting in severe MR, with anteriorly directed jet; MR effective regurgitant area (EROA) is 0.52cm2 and regurgitant volume is 75ml (Figure 1A, 1B & 1C).

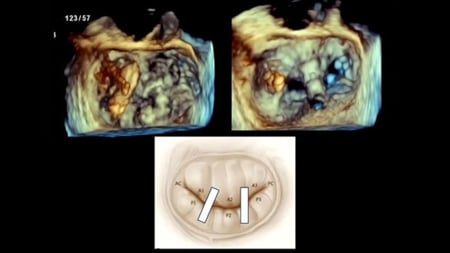
Figure 1. TTE showing double frame view of Apical 4-chamber and color doppler of severe MR and PISA radius measurement (A), Continuous flow wave doppler accross MV (B), transgastric short axis showing fishmouth view and doppler of MV with Prolapse P2 (C), TEE mid esophageal bicaval view showing giant chiari network (D), and transseptal puncture (E), and subsequent dragging of chiari network strand into LA (F), strands of chiari network adhered on the retracted CDS (G), TEE midesophageal bicaval view of re-transeptal puncture and guiding of CDS into LA smoothly (H), new Mitraclip deployed at MV (I), 3d image of MV upon successful deployment of mitraclip (J), Fluoro image post 2nd MItraclip deployment (K), Pulse wave doppler showing immediate normalization of PVF reversal (L).
He was referred to cardiothoracic surgeon and was advised for surgery. However, patient firmly refused invasive surgery. Decision was made for Mitraclip implantation. This case was performed against current guidelines, ignoring the decision of heart team and according only to the wishes of the patient. For this reason, only its technical value should be considered.
Pre-procedural Transesophageal Echo (TEE) (Figure 1D, Moving image 1) showed giant Chiari network in right atrium, which was not observed in TTE. Decision made to proceed with the procedure, as it appeared feasible to avoid dragging the Chiari network across the septum (Moving image 2).
However, after the transseptal puncture (Figure 1E), while advancing the Mitraclip delivery system (CDS) into left atrium (LA), the Chiari network was dragged into LA (Figure 1F, Moving image 3), and upon further advancement of the CDS, the strands of Chiari network clung to the mitraclip (Moving image 4).
Decision was made to tear the Chiari network that clung to the Mitraclip by rotatory, and back-and-forth motion of the delivery catheter and then to retract the Mitraclip and delivery catheter to avoid embolization of Chiari network strands (Moving images 5). Upon removal of the CDS, we noted the strands of Chiari network adhered on the retracted Mitraclip (Figure 1G).
After ensuring that there were no Chiari strands at the mouth of delivery catheter, a new second Mitraclip was then advanced smoothly (Figure 1H), and deployed at A2/P2 (Figure 1I, 1J, Moving image 6), resulted in immediate reduction of MR.
In the presence of small residual flail, another Mitraclip was deployed lateral to the first clip, giving an excellent outcome (Figure 1K). Post procedural TEE shows double mitral inflow orifices with reduction of MR from 4+ to trivial, and normalization of pulmonary vein flow (PVF) reversal (Figure 1L, Moving image 7).
Currently, over 8 years post procedure, patient is well and asymptomatic. Latest TTE shows moderate MR, and absent PVF reversal (Moving image 8).
Mitraclip implantation is usually avoided in the presence of giant Chiari network, as there is a serious concern of catheter device entanglement in the Chiari network and risk of embolization of Chiari strands.
Two case studies reporting giant Chiari network complicating Mitraclip implantation procedures have been published before1, and in both studies the procedures were abandoned. Procedure should be attempted meticulously, however should be abandoned in the event of further perplexity. Pre-procedural TEE is indispensable, for it avoids unnecessary complication and leads to finer patient selections. To the best of our knowledge, this is the first report of successful Mitraclip implantation in a patient with giant Chiari network.
Conflict of interest statement
All authors have no conflict of interest to declare.
Affiliations
- Department of Cardiology, Institut Jantung Negara, 50450 WP Kuala Lumpur, Malaysia.
Reference
- Yeo K.K., Chiam P.T.L., Tan J., and Ding Z.P. (2013) Chiari Network Complicating a MitraClip Procedure. In: Feldman T., Franzen O., Low R., Rogers J., Yeo K. (eds) Atlas of Percutaneous Edge-to-Edge Mitral Valve Repair. Springer, London
1 comment
Great learning lesson. On seeing a pathological valve which is in need of BMV, such structures of lesser importance as chiari networks are often ignored. Deserve a keen eye too!