22 Dec 2020
Multimodality guided management of an unusual case of STEMI
Supported by the EuroIntervention Journal
A 47-year-old woman without previous medical history was admitted for chest pain with ST-segment elevation in the inferolateral leads. Echocardiography showed inferior and infero-lateral wall hypokinesia with preserved global left ventricular function...
Authors
Massimo Fineschi1,2, Tommaso Gori2
Case summary
A 47-year-old woman without previous medical history was admitted for chest pain with ST-segment elevation in the inferolateral leads. Echocardiography showed inferior and inferolateral wall hypokinesia with preserved global left ventricular function. Emergency coronary angiography showed dynamic systolic compression/obstruction in distal right coronary artery (Panel A1-A2).
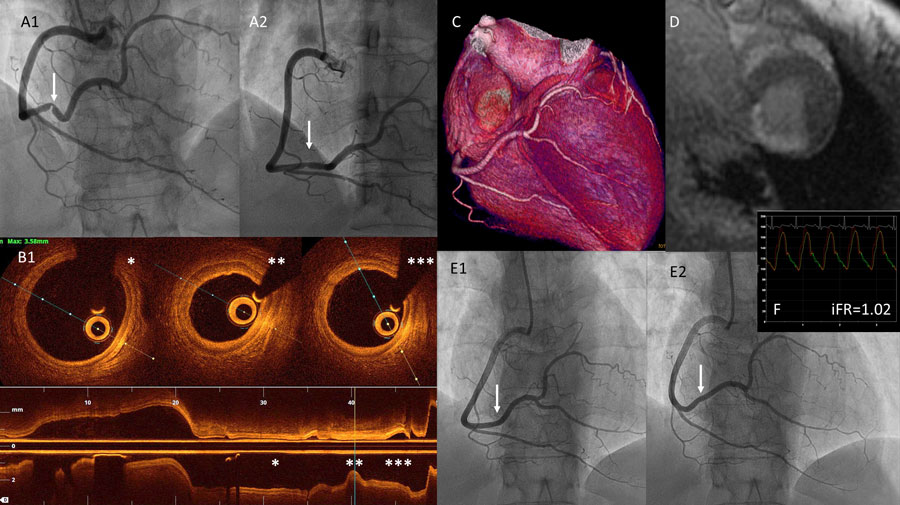
(A1-A2) coronary angiography of the right coronary artery during systole and diastole; (B) OCT distal, proximal and at the culprit lesion; (C) Computed axial tomography; (D) Cardiac magnetic resonance; (E1-E2) coronary angiography of the right coronary artery at follow up during systole and diastole; (F) iFR
Optical coherence tomography did not reveal evidence of plaque disruption, erosion or coronary artery dissection, and there was no evidence suggestive of myocardial bridge. There was intimal and media hyperplasia with a minimal lumen area of 2.8 mm2 (Panel B1-B2-B3). Based on this information, no stent was deemed indicated.
Computed axial tomography excluded the presence of myocardial bridging (Panel C) and cardiac magnetic resonance imaging confirmed transmural delayed enhancement indicative of myocardial necrosis (Panel D). The patient was discharged on dual antiplatelet therapy with aspirin and ticagrelor, calcium channel blocker and statin. At one year follow up, the patient remained asymptomatic; coronary angiography showed a clear regression of the dynamic narrowing (Panel E1-E2). Instantaneous wave-free ratio was =1 (Panel F).
In cases of angiographically ambiguous lesions, despite ST-elevation ECG, intravascular imaging allows optimization of patient care and, in this case, avoids unnecessary stent implantation. Myocardial ischemia with non-obstructive coronary artery disease is a frequent (up to 1/3 of myocardial infarctions in the young) but complex clinical entity. In this case, advanced intracoronary diagnostics was important to exclude plaque dissection/disruption and angiographically silent plaques. There was no evidence suggestive of type II myocardial infarction, Tako-Tsubo cardiomyopathy or myocarditis (anemia, C-reactive protein elevation, late enhancement). Acetylcholine vasospasm testing might have added value but was not used in this case. By exclusion, the most likely explanation for the acute presentation was a mechanical compression/obstruction of the distal right coronary artery due to a hyperkinetic myocardium coupled with a transient focal coronary spasm at the level of a tortuous hinge point.
Conflict of interest statement
The authors do not have conflicts of interest
Affiliations
- U.O.S.A Cardiologia Interventistica, Ospedale S. Maria alle Scotte, Siena, Italy
- Kardiologie I Universitätsmedizin Mainz, Germany
4 comments
Nice Case, the use of appropriate technology clearly helps clinician
The pseudo-lesion observed on baseline angiogram probably was caused by vessel kinking.
Great elaboration with all the available diagnostic modalities .........just a question only for my unfer standing ????? Couldnt this,ve bin a clot causing obstruction and later on having been dislodged ????????
Great elaboration with all the available diagnostic modalities .........just a question only for my unfer standing ????? Couldnt this,ve bin a clot causing obstruction and later on having been dislodged ????????