02 Sep 2024
Simplified dual-indeflator approach for bioprosthetic valve fracture
A problem-solving step by step tutorial
The standard BVF procedure involves multiple quick maneuvers. Simplifying the setup, minimizing operator actions, and shortening rapid pacing could reduce associated risks. Find out how!
Frequency of the problem:
Expert level:
Summary
Bioprosthetic valve fracture (BVF) during valve-in-valve transcatheter aortic valve implantation (ViV-TAVI) is an important technique to optimize the haemodynamic outcomes of the new transcatheter valve1. This method involves using a high-pressure balloon to fracture the rigid frame of a failing surgical bioprosthesis, thereby allowing an effective deployment and expansion of the new transcatheter valve2.
This technique is particularly useful when the bioprosthetic valve has a small internal diameter (≤ 21 mm).
Although generally effective, the procedure carries risks such as prolonged rapid pacing, extended hypotension, ischemic stroke and potential damage to surrounding cardiac structures. Therefore, it requires a quick execution with an operator expertise and simplified procedural set-up1.
The Problem
Standard BVF procedure necessitates several sequential maneuvers within a very short time frame, including:
- Inflating the balloon with a 50 ml syringe while the 3-way stopcock connects the syringe and balloon
- Simultaneously applying forward pressure on syringe and rotating the 3-way stopcock to connect the indeflator and balloon
- Switching to pressure indeflator
- Further inflating the balloon with an indeflator (push and then rotation) until achieving BVF
- Balloon deflation. This multi-step process is demanding and increases required time, thereby introducing the potential for operator error and patient complications (prolonged rapid pacing and extended hypotension)
Principal idea
The principal idea was to simplify the procedural set-up, minimize operator maneuvers, and shorten the duration of rapid pacing. Overall, this could potentially reduce the risks of this procedure. Despite being previously reported in one review article2, this technique has been largely underutilized, to the best of our knowledge.
Material needed
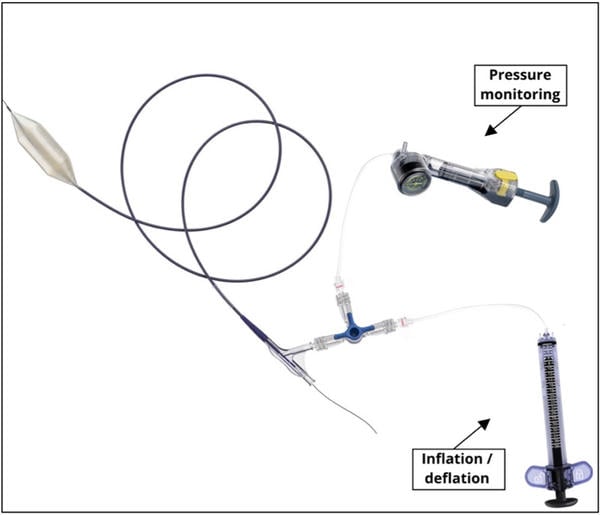
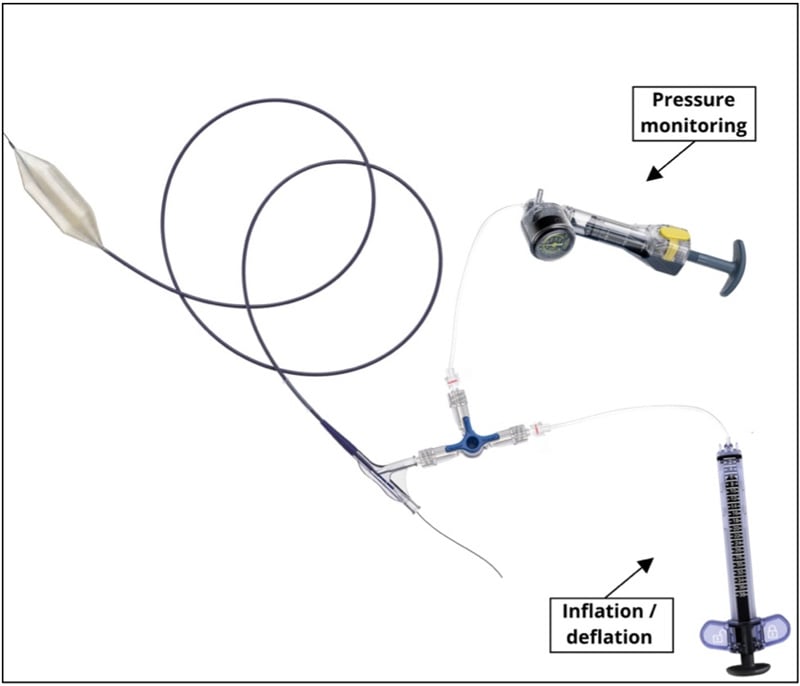
- 1 large volume indeflator – “primary indeflator” (example: Edwards / Atrion QL38®)
- 1 standard indeflator with pressure monitor – “secondary indeflator” (example: any PCI indeflator)
- 3-way stopcock
- 1 high-pressure balloon (Atlas Gold Bard® or True Bard®)
- Contrast-saline mixture (85/15 ratio)
Method step-by-step
Step 1
Standard preparation and de-airing of the high-pressure balloon. Assembly of high-pressure balloon, 3-way stopcock, large volume indeflator and standard indeflator with pressure monitor.
Step 2
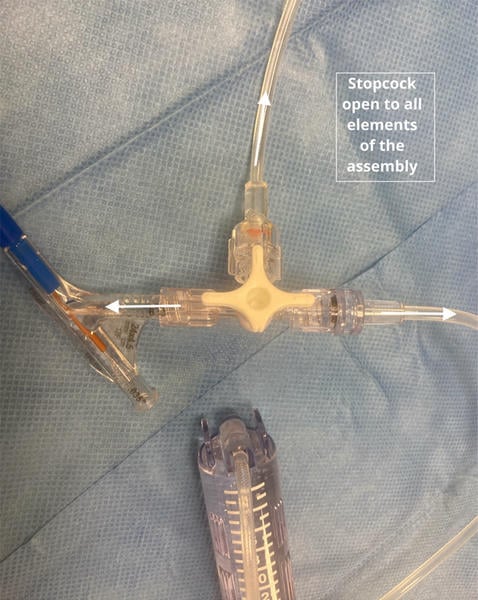
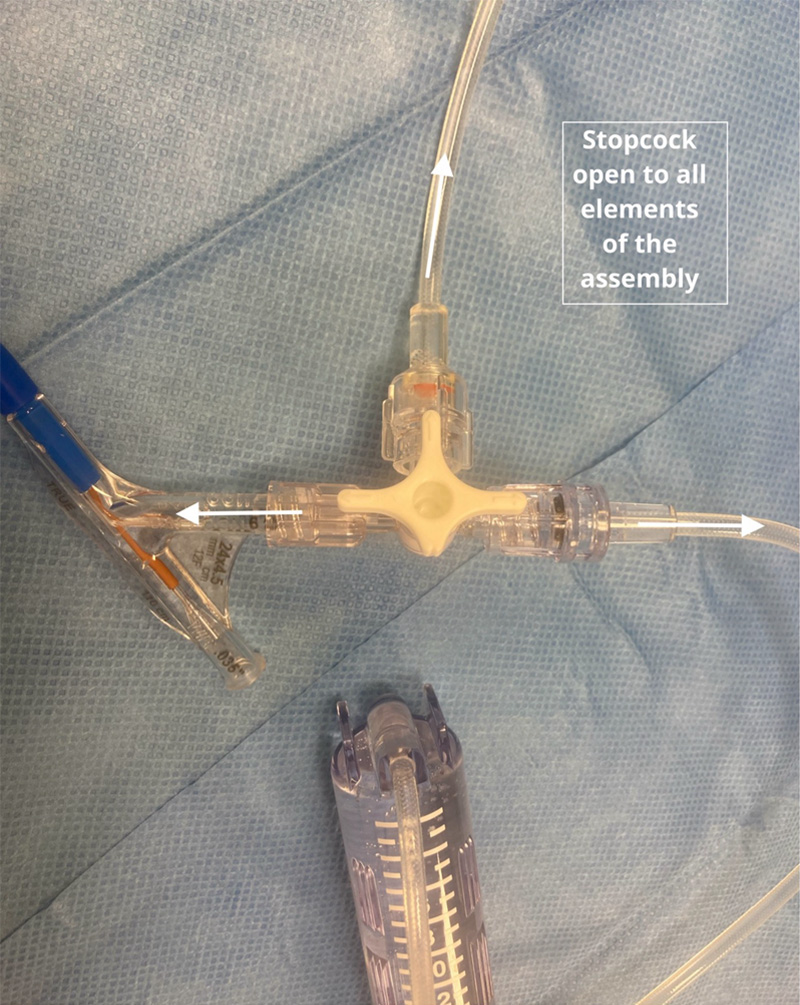
Introduction and positioning of the high-pressure balloon across the surgical bioprosthesis. Reassurance on the position of 3-way stopcock (open in all 3 directions), and de-aired fluid (contrast/saline mixture) filled indeflators.
Step 3 - Bioprosthesis valve fracture
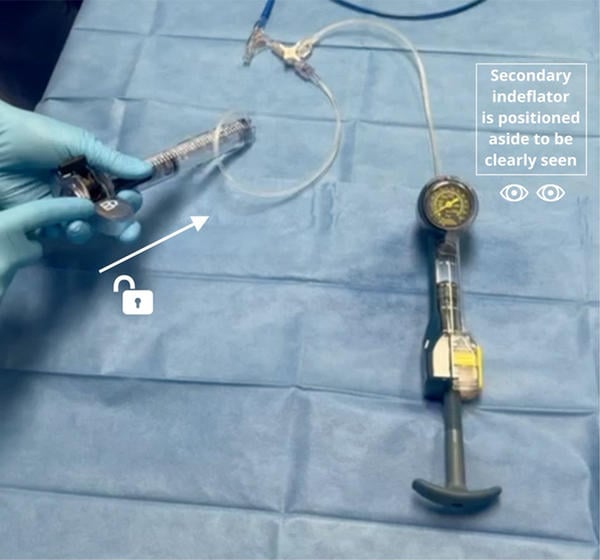
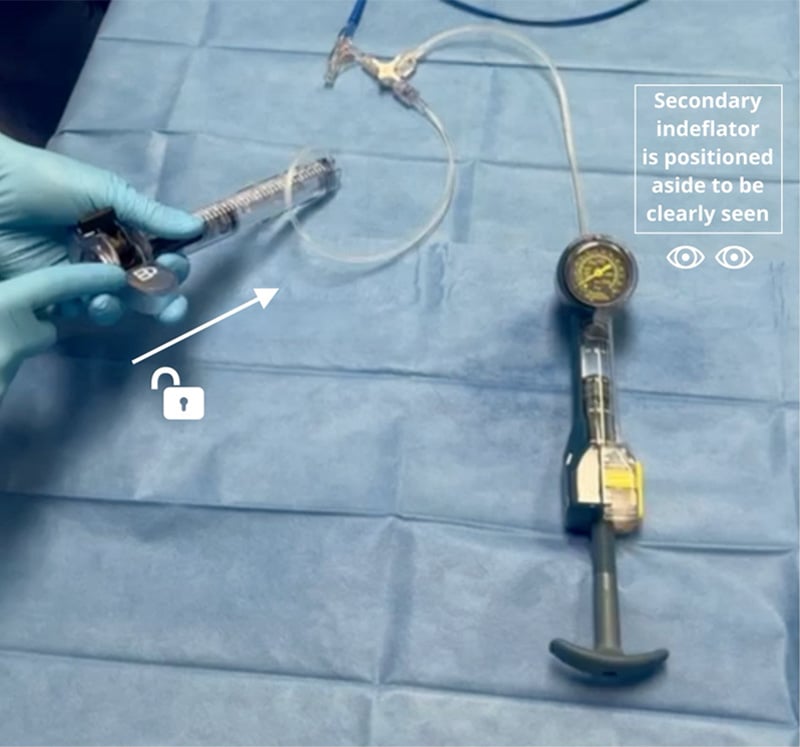
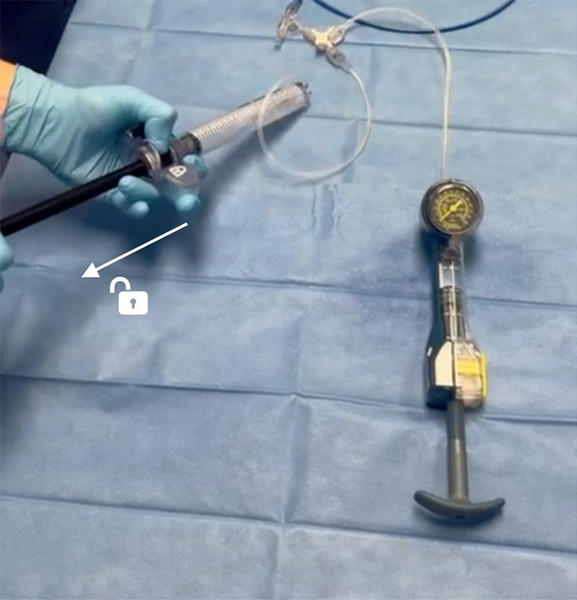
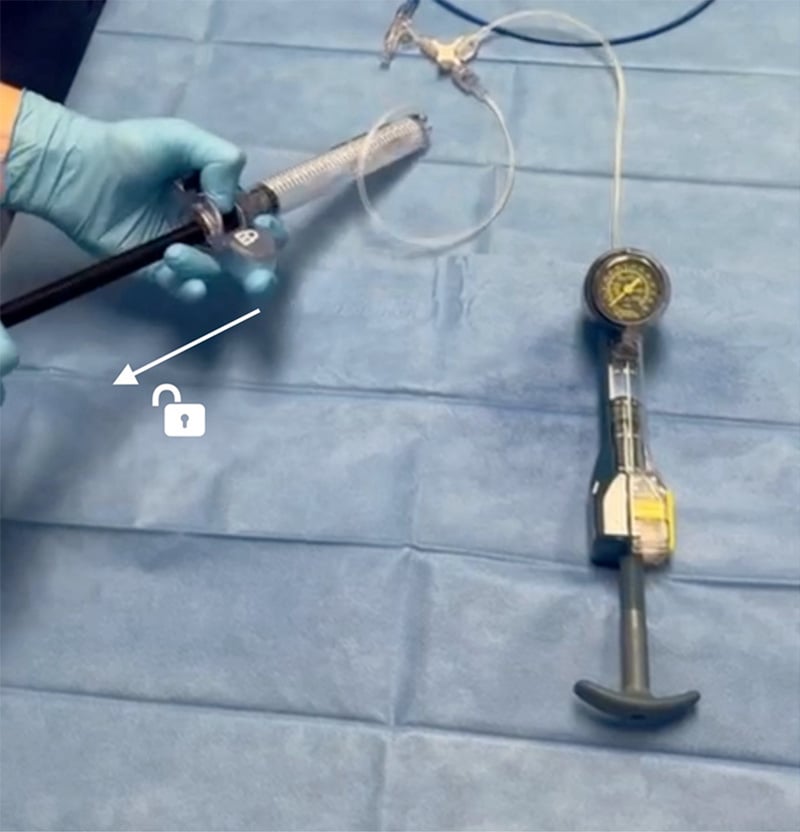
- Step 3a: Manual balloon inflation by pushing the unlocked handle of the large volume “primary indeflator”.
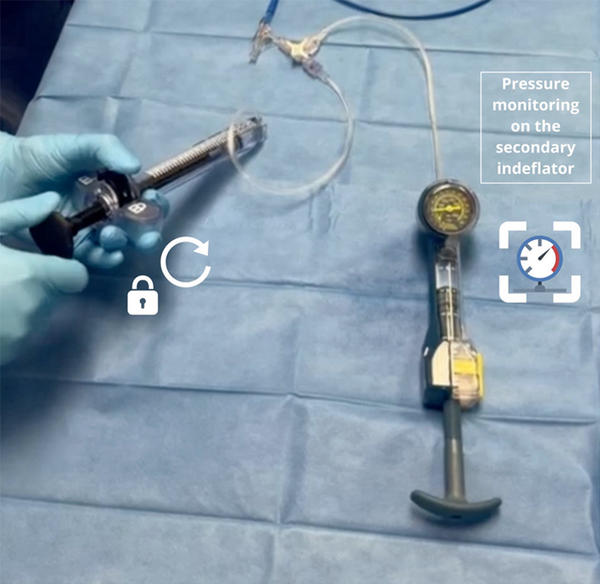
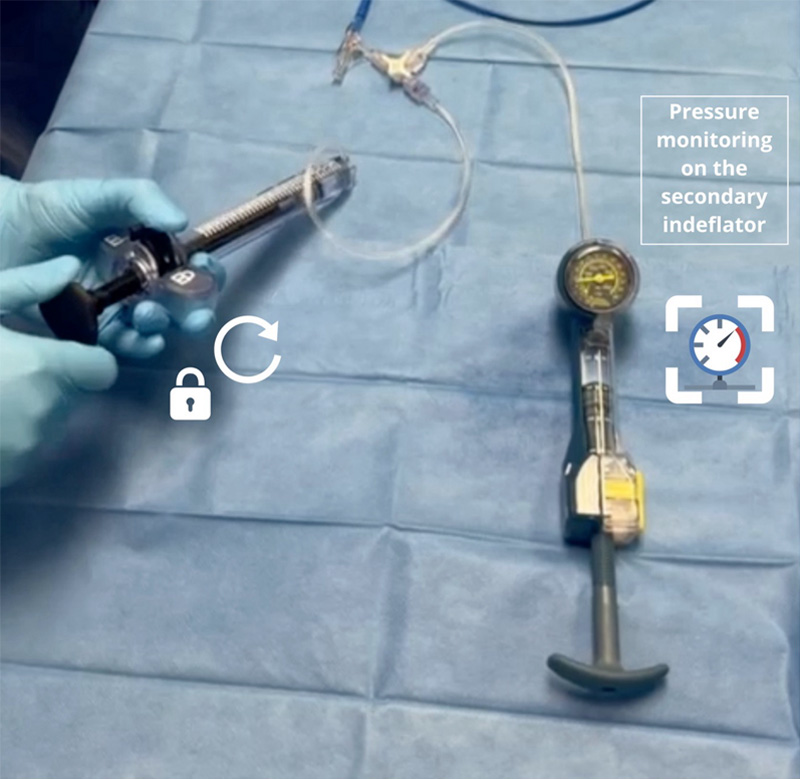
- Step 3b: Manual balloon inflation by rotating the locked handle of the large volume “primary indeflator” and observation of pressure monitor on the standard “secondary indeflator”.
Tip: It is advised that the 3rd operator or a nurse/technician loudly states pressure on the indeflator as it increases.
- Step 3c: Following the BVF (visual and/or pressure confirmation): Manual balloon deflation by pulling the unlocked handle of the large volume “primary indeflator”, followed by handle locking.
Points of specific attention
- De-air the system thoroughly.
- The "primary indeflator" should be completely filled with fluid.
- The "secondary indeflator" with pressure monitor should be partially filled with fluid to allow better pressure conduction, and to leave option of applying additional negative pressure if needed post fracture. Avoid complete fluid filling of "secondary indeflator".
- The "secondary indeflator" should be positioned to be clearly visible.
- It is advised that the one operator or a nurse/technician loudly states pressure on the indeflator as it increases.
- Plan the procedure and know the approximate fracture pressure for specific surgical valve.
A word from the reviewer - Alexander Wolf

BVF is an important technique to optimize hemodynamic results in Valve-in-Valve patients. The proposed use of a primary and secondary indeflator is helpful in reducing rapid pacing time and simplifies team work at the table. Nevertheless, careful case planning and knowledge about the surgical valve (e.g. BVF possible, pressure required to fracture) is crucial.
References:
- Hashimoto G, et al. New Insights and Perspective on Bioprosthetic Valve Fracture From Bench Testing and Computed Tomography Analysis. Struct Heart. 2024;8(3):100276. doi: 10.1016/j.shj.2023.100276.
- Sreedharan et al. Bioprosthetic Valve Fracture to Facilitate Valve-in-Valve Transcatheter Aortic Valve Replacement. Structural Heart. 2021;5(1):24-30. doi: 10.1080/24748706.2020.1844354.
Authors





1 comment
Even smaller (0-5%) contrast percentage facilitates recognition of stent fracture on fluoroscopy and theoretically reduces gradient pressure in the balloon shaft. For safety of this approach, CT analysis should prove uncalcified STJ with a diameter larger than the planned NC balloon diameter. Thank you for sharing and beautiful presentation of such a useful technique!