STOPDAPT-2 ACS: exploring the limits of short DAPT
Reported from the European Society of Cardiology ESC Congress 2021
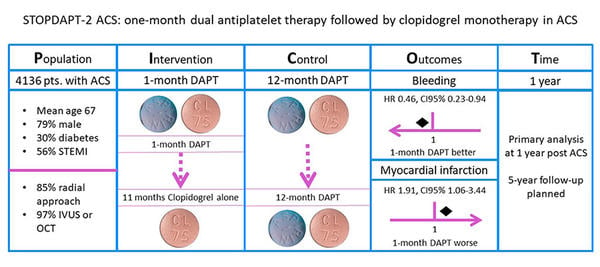
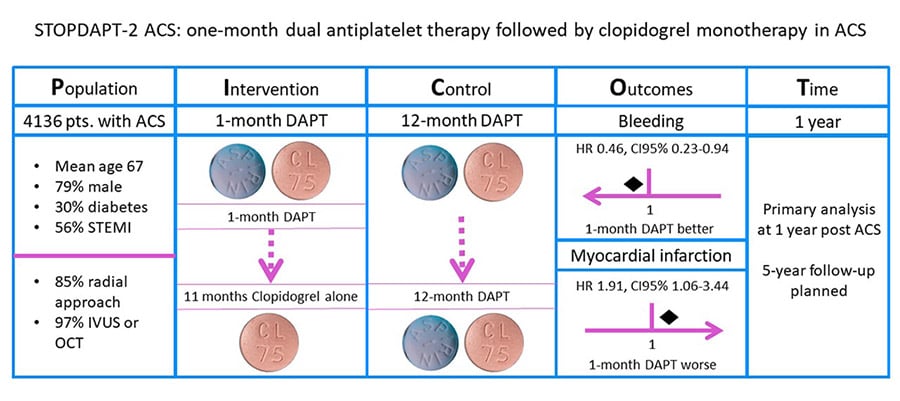
Following presentation of the results of the MASTER-DAPT trial, the main message appears to have been that short DAPT could reduce bleeding at no additional cost in terms of ischemic events. Hirotoshi Watanabe presented the primary analysis of the STOPDAPT-2 ACS trial (Table), which may highlight the limits of an abbreviated DAPT regimen.
Analysis according to the PICOT principle - courtesy of Dejan Milasinovic
Apart from the fundamental difference in enrolled patient populations, high-bleeding risk (MASTER DAPT) versus acute coronary syndrome (STOPDAPT-2 ACS), both studies used hierarchical testing to prove non-inferiority of short DAPT in terms of ischemic events, prioritising it over a superiority comparison of bleeding rates.
In the STOPDAPT-2 ACS trial, 1-month of clopidogrel-based DAPT with subsequent 11 months of clopidogrel monotherapy did not pass the test of non-inferiority as compared with 12 months clopidogrel-based DAPT for the net combined primary endpoint of CV death, MI, stent thrombosis, stroke and TIMI major/minor bleeding.
Ultimately, short DAPT was associated with a lower incidence of BARC 3/5 bleeding (0.54 % vs. 1.31 %), albeit at the cost of increasing the risk of MI (1.59 % vs. 0.85 %). Of note, an increased risk of MI with short DAPT in ACS patients was already previously documented in the SMART-DATE trial.
Taken together, when translating these results into everyday clinical practice, there are at least the following 3 issues to be considered.
- While the current guideline recommendation to maintain 12-month DAPT in ACS patients seems to be reinforced, one should bear in mind that a clinical setting of high-bleeding risk (HBR) in ACS was not explored in the STOPDAPT-2 ACS study.
- The overall event rates appear to be low. This may signal that the population included was low-risk for both bleeding and ischemic events. Clinically challenging settings such as overlapping of high bleeding and ischemic risk are not informed by the results of the STOPDAPT-2 trial.
- Post hoc analyses of the GLOBAL LEADERS and TWILIGHT trials indicated that Ticagrelor monotherapy may reduce bleeding compared with Ticagrelor-based DAPT, without increasing the risk of ischemic events even in patients with ACS. Hence, a more potent (and reliable) P2Y12 inhibition may open the door towards an abbreviated course of DAPT in at least a subgroup of patients with ACS in the future.
In summary, the main lesson appears to be that, in the current practice, there are limits to how far we can go in shortening DAPT. Specifically, Clopidogrel monotherapy after only one month of DAPT appears to be inadequate for most ACS patients, even with nearly 100 % utilization of intracoronary imaging guidance to optimize PCI results as seen in the STOPDAPT-2 ACS trial.

No comments yet!