FFR-guided PCI optimization directed by high-definition IVUS versus standard of care - the FFR-REACT trial
Selected in JACC: Cardiovascular Interventions by S. Fezzi , M. Pighi
The primary objective of the study was to assess whether an IVUS-based stent optimization provided an incremental value in terms of vessel-related adverse event occurrence in patients presenting with low post-PCI FFR (<0.90).
References
Authors
Tara Neleman, Laurens J.C. van Zandvoort, Maria N. Tovar Forero, Kaneshka Masdjedi, Jurgen M.R. Ligthart, Karen T. Witberg, Frederik T.W. Groenland, Paul Cummins, Mattie J. Lenzen, Eric Boersma, Rutger-Jan Nuis, Wijnand K. den Dekker, Roberto Diletti, Jeroen Wilschut, Felix Zijlstra, Nicolas M. Van Mieghem, and Joost Daemen
Reference
J Am Coll Cardiol Intv. 2022 Aug, 15 (16) 1595–1607
Published
22 August 2022
Link
https://www.jacc.org/doi/10.1016/j.jcin.2022.06.018Reviewers


Our Comment
Why this study – the rationale/objective?
Suboptimal physiological result, despite successful angiographic PCI, is common (20-30 %), and may have an impact on clinical events, mainly vessel-oriented. Post-PCI FFR has been shown to be increased by additional stenting or post-dilatation.
Nevertheless, previous studies were not powered for the assessment of the impact on hard clinical outcomes and did not take into account the combined intracoronary imaging analysis. Thus, whether an IVUS-based PCI optimization approach, with improvement of post-PCI physiology assessment, is related with better outcomes, remains unknown.
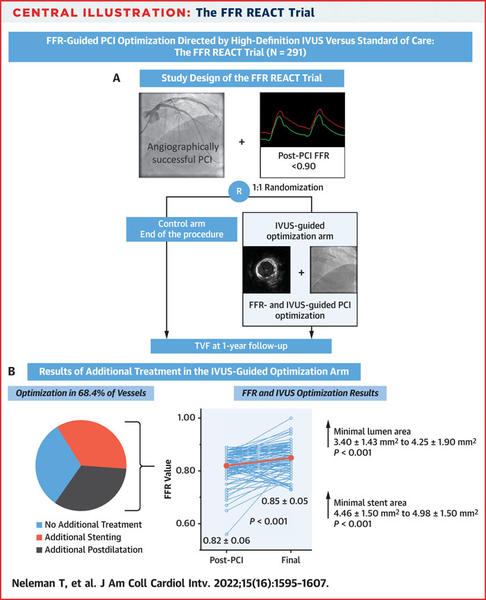
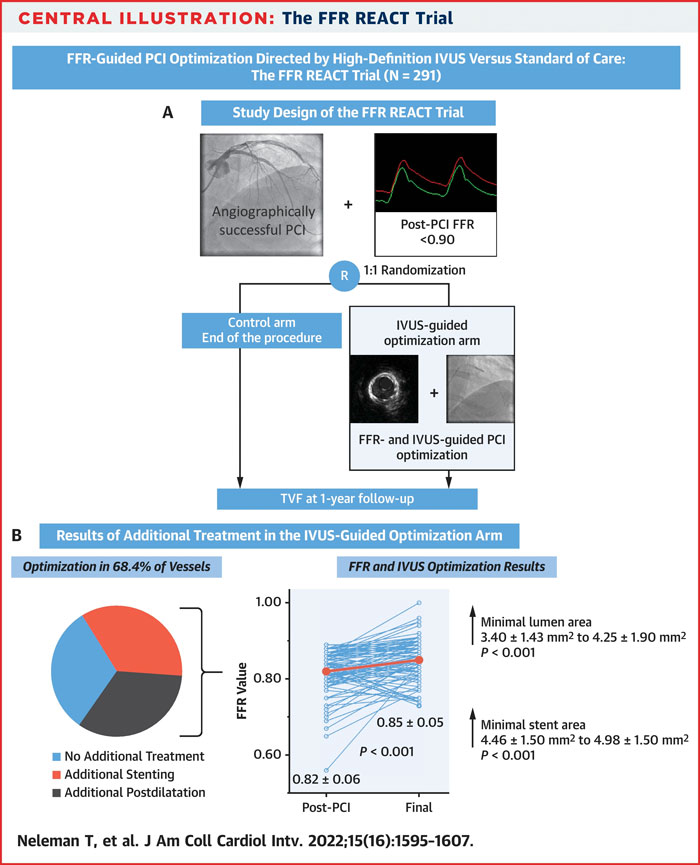
The FFR REACT was a single-center, randomized, double-blind, parallel-arm trial that prospectively allocated patients with post-PCI suboptimal result (FFR < 0.90), either to an IVUS-guided PCI optimization (intervention group), or to standard of care (control group), in a 1:1 ratio.
The primary objective of the study was to assess whether an IVUS-based stent optimization provided an incremental value in terms of vessel-related adverse event occurrence in patients presenting with low post-PCI FFR (<0.90).
How was it executed – the methodology?
- FFR REACT was a single-center, randomized, double-blind, parallel-arm prospective trial that included stable patients that underwent angiographic successful PCI. Patients presenting with STEMI < 72H, small vessels, or cardiogenic shock were excluded.
- Blinded FFR assessment was performed after angiographically successful PCI in 621 patients: 291 presented with a low post-PCI FFR value (< 0.90) and underwent randomization to IVUS-guided optimization (n = 145) or control (n = 146).
- FFR was measured through a microcatheter (Navvus, ACIST Medical Systems, Inc) distally to the stenosis, at the distal and proximal edge of the stent, and at the coronary ostium. Hyperemia was induced by intravenous infusion of adenosine.
- IVUS-based optimization was based on a standardized protocol. Three different optimization patterns were distinguished: post-dilatation only (1), additional stenting without optimization of the initial stent (2), and additional stenting in combination with initial stent optimization (3).
- The primary endpoint of the study was to compare the incidence of target vessel failure at 12 months, defined as a composite occurrence of cardiac death, spontaneous target vessel myocardial infarction, and clinically driven target vessel revascularization (CD-TVR) between patients with low post-PCI FFR values undergoing an IVUS-based optimization and the control group that did not receive further interventions.
The FFR REACT Trial
Source = JACC: Cardiovascular Interventions
What is the main result?
- Patients randomized to the IVUS-guided optimization arm presented with a higher baseline complexity in terms of clinical (more frequently diabetic, with previous stroke and with lower LVEF) and procedural variables (higher number of stent implanted, longer total stent length, higher prevalence of lesion type B2/C, CTO and lower post-PCI FFR).
- In the IVUS-guided optimization arm, stent underexpansion was reported in 62.2 % of the stents, residual focal lesions proximally or distally to the stent in 30.8 %, while only 9.1 % of the cases met all the optimal stenting criteria.
- A total of 104 (68.4 %) vessels in the IVUS-guided optimization arm underwent additional optimization including additional stenting (34.9 %) or post-dilatation only (33.6 %).
- Stent optimization led to a mean increase in post-PCI FFR (from 0.82 ± 0.06 to 0.85 ± 0.05 (P < 0.001)) and in post-PCI FFR > 0.90 rate (from 0 to 20 % of the vessels).
- The incidence of 1-year TVF was comparable between the 2 study arms (IVUS-guided optimization arm: 4.2 %, control arm: 4.8 %; P = 0.79). Whereas a trend towards higher incidence of cardiac death was seen in the IVUS group (HR 4.06; CI 95 % 0.45-36.34; p = 0.17), a trend toward a lower incidence of clinically driven target vessel revascularization in the IVUS-guided optimization arm was also reported (0.7 % vs. 4.2 %, P = 0.06).
Critical reading and relevance for clinical practice
This report builds up the evidence on the importance of post-PCI physiological evaluation and aims at providing an imaging-based optimization strategy to improve clinical outcomes.
However, the low rate of adverse events has limited the inferential power of the study, showing that an IVUS-guided optimization strategy in response to post-PCI FFR < 0.90 did not affect the 1-year TVF rate compared with the standard of care.
The study showed improved physiological outcomes and increased luminal areas albeit without an improved clinical benefit.
To date, physiology evaluation following an apparently successful angio-guided PCI remains underused (less than 10 %), mainly due to technical and economic reasons, prolonging procedural times, and requiring the administration of hyperaemic agents when FFR is used.
However, suboptimal physiological results are observed in up to 30 % of the cases, with LAD location (three out of four of the cases in the present manuscript), low baseline FFR, and the presence of diffuse disease associated with an increased risk.
Combined physiology-intracoronary imaging studies have outlined as several stent-related factors, such as geographical miss of the plaque, stent malapposition, underexpansion, major edge dissections as well as plaque or thrombus in-stent prolapse, are prone to a residual physiological drop after PCI.
However, besides several retrospective analyses, only few prospective studies (FFR-SEARCH, HAWKEYE trial) are available and have suggested a significant relationship between post-PCI physiology and clinical outcomes, mainly related to vessel-oriented outcomes. Indeed, the prospective FFR-SEARCH study failed to show an increased risk of MACE in case of post-PCI < 0.90.
The DEFINE-PCI study has suggested that post-PCI iFR < 0.95, besides being a common finding (> 60 %), significantly impacts on clinical outcomes and residual angina. In this view, the pressure pullback seems to represent a key tool in defining the underlying problem and consequent needed intervention. Based on pressure-wire pullback assessment, in the 1:1 randomized TARGET-FFR trial a physiology-guided incremental optimization strategy even without showing a significant increase in the proportion of patients with a final FFR >0.90 (in a similar way to the FFR-REACT trial), showed a reduction in the proportion of patients with a final FFR<0.80.
Diffuse disease is possibly associated with suboptimal FFR value after IVUS-directed PCI seen in the present study, as it still represents a conundrum, with suboptimal PCI results requiring long-stented segments with the risk of side-branch occlusion and vascular caging. In this view, the targeted physiologic parameter or endpoint should be decided before the PCI procedure, through physiological pattern of disease assessment.
Non-hyperemic pressure indexes, angiography-derived (iFR, QFR, FFRangio, and vFFR), and intracoronary imaging (OFR, UFR) may offer additional information to define the exact location and mechanism of suboptimal post-PCI physiology results allowing to precisely allocate a patient-tailored treatment (i.e., conservative medical therapy or additional PCI), having the inherited advantage of physiology-angiography coregistration. These advantages might be of particular importance, especially in complex lesions, diffuse or serial disease.
References:
- Kikuta Y, Cook CM, Sharp ASP, et al (2018) Pre-Angioplasty Instantaneous Wave-Free Ratio Pullback Predicts Hemodynamic Outcome In Humans With Coronary Artery Disease: Primary Results of the International Multicenter iFR GRADIENT Registry. JACC Cardiovasc Interv 11:757–767.
- Scarsini R, Fezzi S, Pesarini G, et al. Impact of physiologically diffuse versus focal pattern of coronary disease on quantitative flow reserve diagnostic accuracy. Catheter Cardiovasc Interv 2022; 99(3):736-745.
- Jeremias A, Davies JE, Maehara A, et al. Blinded Physiological Assessment of Residual Ischemia After Successful Angiographic Percutaneous Coronary Intervention: The DEFINE PCI Study. JACC Cardiovasc Interv 2019; 12: 1991–2001.
- Ding D, Huang J, Westra J, et al (2021) Immediate post-procedural functional assessment of percutaneous coronary intervention: current evidence and future directions. Eur Heart J 353:1–16.
- Biscaglia S, Tebaldi M, Brugaletta S, et al. Prognostic Value of QFR Measured Immediately After Successful Stent Implantation: The International Multicenter Prospective HAWKEYE Study. JACC Cardiovasc Interv 2019; 12: 2079–88.
- Van Zandvoort LJC, Masdjedi K, Witberg K, et al. Explanation of postprocedural fractional flow reserve below 0.85: A comprehensive ultrasound analysis of the FFR SEARCH registry. Circ Cardiovasc Interv 2019; 12: 1–10.
- Diletti R, Masdjedi K, Daemen J, et al. Impact of Poststenting Fractional Flow Reserve on Long-Term Clinical Outcomes: The FFR-SEARCH Study. Circ Cardiovasc Interv 2021; : 314–22.
- Damien Collison, Matthaios Didagelos, Muhammad Aetesam-ur-Rahman et al. Post-stenting fractional flow reserve vs coronary angiography for optimization of percutaneous coronary intervention (TARGET-FFR), European Heart Journal, Volume 42, Issue 45, 1 December 2021, Pages 4656–4668.
No comments yet!