International hand function study following distal radial access: the RATATOUILLE study
Selected in JACC: Cardiovascular Interventions by A. Cader , S. R. Khan
This trial aimed to evaluate hand function following distal radial approach coronary angiography or percutaneous coronary intervention, to assess longer term safety of the technique.
References
Authors
Gregory A. Sgueglia, Ahmed Hassan, Stefan Harb, Tom J. Ford, Leonidas Koliastasis, Anastasios Milkas, Dimitri M. Zappi, Andrés Navarro Lecaro, Eugenio Ionescu, Stephen Rankin, Christian F. Said, Bibi Kuiper, and Ferdinand Kiemeneij
Reference
JACC Cardiovasc Interv . 2022 May 9 ; S1936-8798(22)00841-X. doi: 10.1016/j.jcin.2022.04.023.
Published
09 May 2022
Link
Read the abstract
Reviewers


Our Comment
Why this study – the rationale/objective?
The distal radial access (DRA) is gaining increasing popularity as an alternative to conventional transradial access (TRA), given its improved procedure ergonomics for the patient and reduced rates of radial artery occlusion (RAO)1,2.
However, the effects of distal radial puncture, wiring, sheath insertion, and haemostatic compression for hand dysfunction, including nerve or tendon injury, have not been previously assessed.
The RATATOUILLE trial aimed to evaluate hand function following DRA coronary angiography or percutaneous coronary intervention, to assess longer term safety of the technique3.
How was it executed - the methodology
Design:
Investigator-driven, prospective, multicentre, international, cohort study.
Inclusion criteria:
Adult patients > 18 years of age with clinical indication of percutaneous coronary procedure and a palpable distal radial artery with orthodromic flow showed by Doppler ultrasound.
Exclusion criteria:
- mandatory indication to another access
- enrolment in a competing or interfering clinical study
- a clinical condition certainly limiting pre- and post-procedural assessments and follow-up.
DRA techniques & operator eligibility:
DRA was performed according to standard protocol. Ultrasound guidance was recommended. Operators were required to have adequate experience with > 50 DRA procedures as primary operator.
Haemostasis was performed according to local practice, aiming at the lowest possible pressure and shortest possible time.
Hand function assessment:
Hand function was defined as the capacity to use the hand in everyday activities depending on anatomical integrity, sensation, coordination, strength, and dexterity4.
Hand function was assessed in a multimodality framework as follows:
- Two validated multidomain questionnaires of self-reported sensibility, weakness, and functional status, where a higher score indicates greater disability or discomfort:
- Disabilities of the Arm, Shoulder, and Hand (DASH) questionnaire
- Levine-Katz questionnaire
- Motor function by the Pinch grip test
- Sensory function by the Semmes- Weinstein monofilament test (Baseline Tactile Monofilament; Fabrication Enterprises)
Motor and sensory tests were performed on both hands
Endpoints:
Multiple independent primary endpoints included change from baseline to first available follow-up of the above 4 domains of hand function assessment: DASH and Levine-Katz questionnaire scores, pinch strength, and somatosensory threshold.
Bleeding and RAO were also documented.
Follow-up:
Hand function assessment was performed at pre-procedural baseline and subsequently planned at 1-month, 6-month, and 12-month follow-up, which was hampered by the COVID19 pandemic.
Clinical evaluation and vascular ultrasound to check for distal and forearm RAO were done prior to discharge and at scheduled follow-up time points.
What is the main result?
Overall, 321 patients were included from 9 international centres in Europe, South America, and Oceania.
Follow-up data for analysis was available for 313 patients (70.3 % men, 66 ± 10 years of age).
Left and right DRA were obtained in 54 % and 46 % respectively.
Ultrasound was used to guide puncture in 85 % of cases.
In 10.9 % patients, DRA was ipsilateral to previous conventional TRA.
99.4 % were hydrophilic sheaths, with sheath size of 5 or 6 French in ~ 80 %.
Haemostasis was achieved with an inflatable device in 81.5 % of patients, and by manual compression in 18.5 %.
Mean haemostasis duration was in 123 ± 75 minutes.
Patient-reported outcomes:
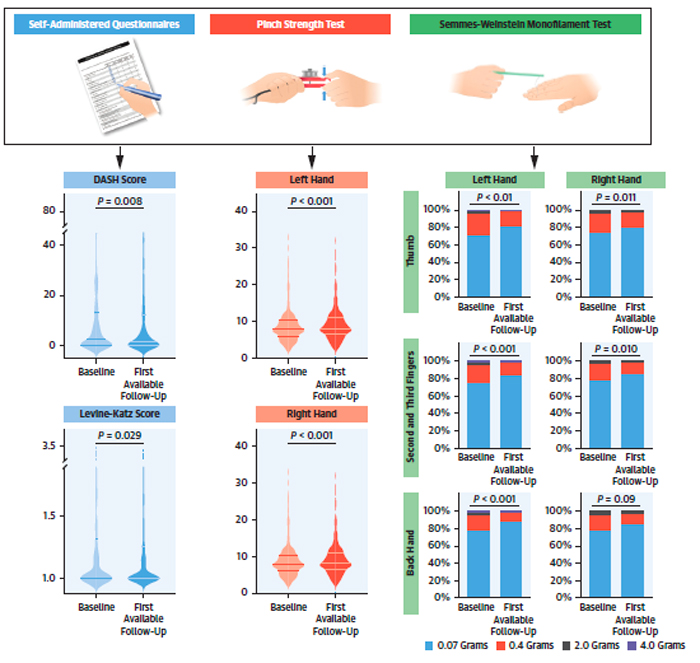
The DASH and the Levine-Katz scores both slightly improved from baseline to follow-up with statistical significance.
DASH score changed from 2.5 (IQR: 0.0-13.3) at baseline to 1.7 (IQR: 0.0-12.5) at follow-up (P = 0.008).
Likewise, the Levine-Katz score changed from 1.00 (IQR: 1.00-1.32) to 1.0 (IQR: 1.00- 1.26); p = 0.029.
A positive correlation was found between the 2 scores (r= 0.48, P < 0.001).
Motor and sensory assessments:
Pinch strength mildly improved from baseline to first available follow-up in both the DRA hand and the contralateral one (P < 0.001 in both cases), with no significant difference between them: + 3.4 % in the DRA hand and + 3.6 % in the contralateral one (P = 0.10).
Significant pinch strength worsening occurred in 20 (6.4 %) cases in the DRA hand, and in 26 (8.3 %) cases in the contralateral hand, with no significant differences between them (P = 0.70).
The touch pressure threshold also appeared to faintly improve in both the left and right hands (P < 0.012 for all the sites).
For both motor and sensory function tests, no significant differences were found for the DRA hand and the contralateral one.
Repeated assessment of all tests over all follow-up time points similarly showed a lack of worsening hand function.
Post-procedure, the self-reported access-related pain assessment according to visual analog scale was 1 (IQR: 0-2).
Access-related adverse events included 19 harmless bleeds.
A single hand swelling was noted, associated with transitory worsening of hand function which recovered by 6 months.
At longest follow-up, 3 patients showed RAO following DRA (forearm and distal RAO, n = 2; isolated distal RAO, n = 1).
An additional isolated forearm RAO was observed in a patient after a second coronary procedure through conventional TRA.
There was no association between RAO and worsening hand function.
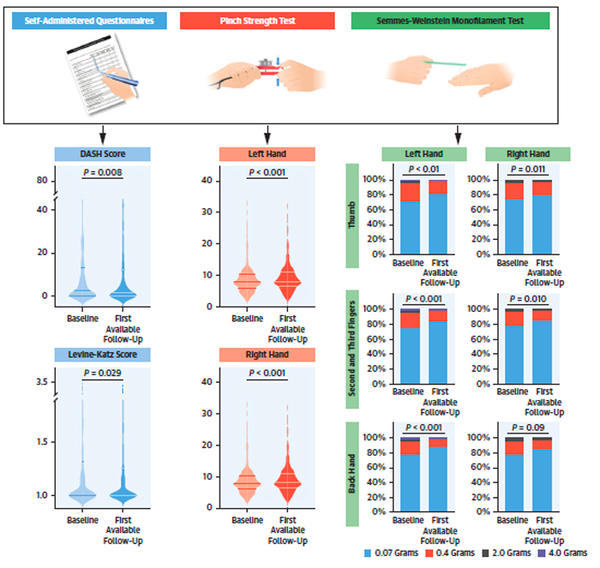
Baseline and post-DRA follow-up evaluations of Disabilities of the Arm, Shoulder and Hand [DASH] and Levine-Katz, motor (pinch grip test), and sensory (Semmes-Weinstein monofilaments test) examinations.
Source = JACC: Cardiovascular Interventions
Critical reading and the relevance for clinical practice
This large multinational real-world DRA registry provides useful observational evidence of the safety of DRA in that it does not impair hand function, as assessed by repeated systematic multidimensional evaluation implementing both subjective and objective assessments, including both motor and sensory function.
The effect of DRA on hand function is an important research question for many reasons: the distal radial artery is smaller than the forearm traditional radial artery, with a less predictable course. This might potentially require multiple punctures, whose effect of direct damage to surrounding nerves and tendons is not known. Furthermore, the consequences of haemostatic compression at the puncture site, effects of haematomas / oedema or ischaemia owing to RAO may also impact hand function.
Although this was an observational cohort and therefore lacks a control group, the authors justify the objectives of this study as one to confirm or exclude hand dysfunction following DRA, as opposed to testing for differences with TRA. Similar to a trial of hand function following TRA5, replication of the assessments at multiple time points did not show worsening of hand function after DRA. Contrary to the TRA study however, patient-perceived access-related pain in RATATOUILLE was half as that reported after conventional TRA, possibly owing to fewer sensory nerve endings on the dorsum.
Although multiple independent primary outcomes spanning across 4 domains were assessed, two of these were patient-reported questionnaires, which albeit validated, render them to the inherent bias of self-reported outcomes, reflecting the subjectivity of responses dependent on a number of factors. Some assessments of hand function, paradoxically, reported clinically relevant mild improvements over time, which the authors attribute to a practice effect.
This was compensated by the pinch grip and Semmes-Weinstein monofilament tests, which provided for more objective assessment of hand function or motor and sensory domains respectively. Furthermore, performing these two tests on both the DRA side and the contralateral side for each patient, provided for an intelligent design with a perfectly matched control measure.
The fact that DRA does not impair hand function on a multi-domain assessment, even where the operator eligibility was just 50 cases and over, is encouraging in terms of safety.
And finally, this study found remarkably low levels of RAO following DRA, further establishing the safety of this access route.
References
- Eid-Lidt G, Rivera Rodriguez A, Jimenez Castellanos J, et al. Distal Radial Artery Approach to Prevent Radial Artery Occlusion Trial. J Am Coll Cardiol Intv. 2021;14:378–385.
- Tsigkas G, Papageorgiou A, Moulias A, et al. Distal or traditional transradial access site for coronary procedures: a single-center, randomized study. J Am Coll Cardiol Intv. 2022;15:22–32.
- Sgueglia GA, Hassan A, Harb S, et al. International Hand Function Study Following Distal Radial Access: The RATATOUILLE Study. JACC Cardiovasc Interv. 2022:S1936-8798(22)00841-X
- Duruöz MT. Assessment of hand function. In: Duruöz MT, ed. Hand Function - A Practical Guide to Assessment. 2nd ed. Springer; 2019:43.
- van Leeuwen MA, van der Heijden DJ, Hermie J, et al. The long-term effect of transradial coronary catheterisation on upper limb function. EuroIntervention. 2017;12:1766–1772.


No comments yet!