Intravascular lithotripsy in comparison to rotational atherectomy for calcified lesions: the ICARE OFDI randomised trial
Selected in EuroIntervention Journal by E. Gallinoro
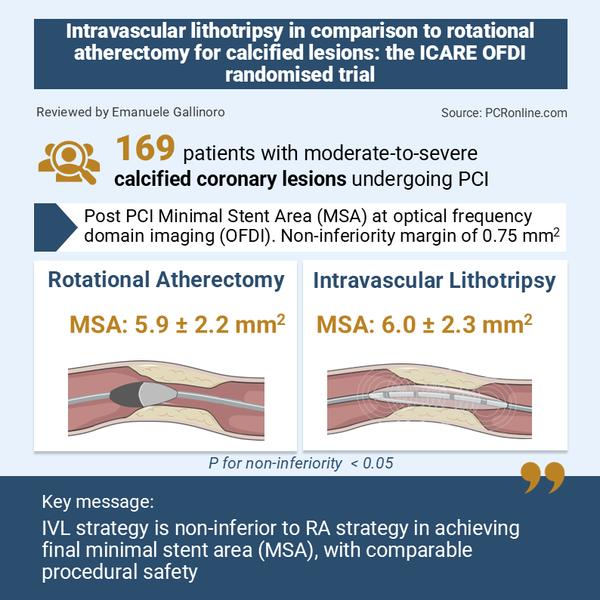
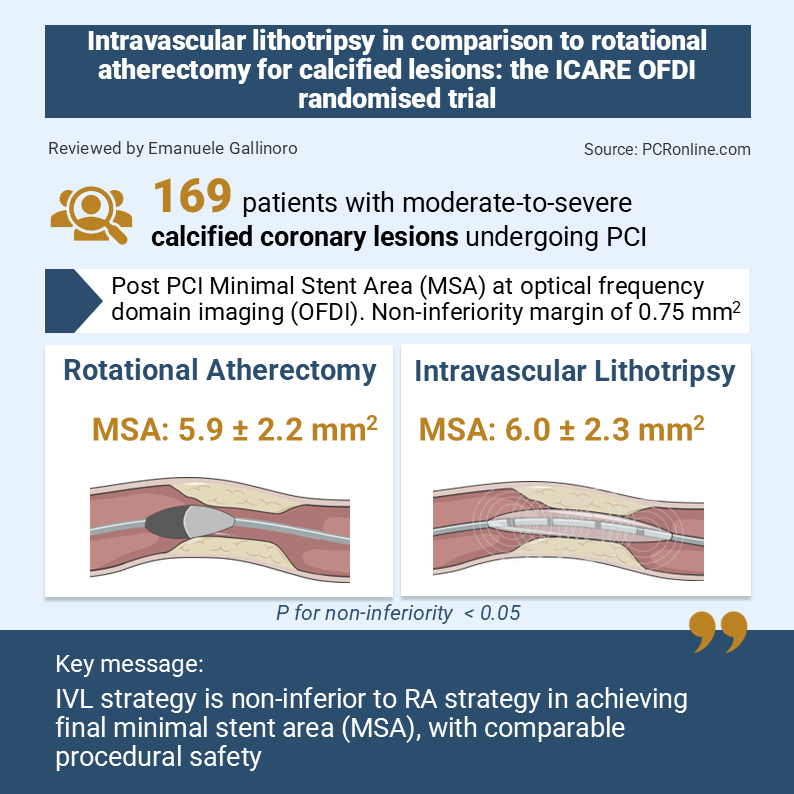
In patients with moderate-to-severe calcified coronary lesions, ICARE OFDI evaluates IVL versus rotational atherectomy as lesion preparation strategies, with OFDI-based assessment of stent results.
References
Authors
Benjamin Honton ; Pascal Motreff ; Jean-Sébastien Mallet ; Thomas Hovasse ; Matthieu Godin ; Guilhem Malclès ; Jerome Brunet ; Nicolas Meneveau ;Pierre Deharo ;Benoit Lattuca ; Erwan Bressollette ; Michael Angioi ; Hakim Benamer ; Edouard Gerbaud ;Bruno Pereira ; Vincenzo Cesario ;Antoine Poinas ; Clémence Laperche ; Antoine Sauguet ; Géraud Souteyrand ; Nicolas Amabile ; Nicolas Combaret
Reference
DOI: 10.4244/EIJ-D-26-00426
Published
May 19, 2026
Link
Read the abstractReviewer

My Comment
Why this study – the rationale/objective?
Severely calcified coronary lesions remain one of the most challenging scenarios in contemporary percutaneous coronary intervention (PCI), being associated with impaired stent expansion, increased procedural complexity, and worse long-term clinical outcomes.
Rotational atherectomy (RA) has historically represented the reference technique for plaque modification in heavily calcified lesions, particularly in uncrossable or highly resistant stenoses. More recently, intravascular lithotripsy (IVL) has emerged as an alternative strategy by fracturing both superficial and deep calcium through acoustic pressure waves delivered by a balloon-based device.
Although observational studies and small randomised trials suggested comparable procedural efficacy between both approaches, the relative role of IVL and RA within contemporary calcium modification strategies remained uncertain and not adequately investigated in randomised studies.
How was it executed? The methodology
The ICARE OFDI trial was a prospective, multicentre, randomised, non-inferiority trial comparing IVL- and RA-based plaque preparation strategies in patients undergoing PCI for moderate-to-severe calcified coronary lesions. A total of 169 patients were randomised to RA (n=86) or IVL (n=83). All procedures were systematically guided by optical frequency domain imaging (OFDI).
Importantly, lesions had to be crossable with a 2.0 mm balloon before randomisation, thereby ensuring technical feasibility of both strategies. The primary endpoint was minimal stent area (MSA) after stent implantation assessed by OFDI (non-inferiority margin set at 0.75 mm2). Secondary imaging endpoints included stent expansion, major malapposition, and procedural complications, while target lesion failure (TLF) was evaluated at 12 months.
The trial was designed as a mechanistic imaging study and was not powered for clinical outcomes.
What is the main result?
IVL was non-inferior to RA for the primary endpoint, with similar final MSA between groups (6.0 ± 2.3 mm² vs 5.9 ± 2.2 mm²; p for non-inferiority < 0.05). Adequate geometrical stent expansion was comparable in both arms (65.1 % vs 65.1 %). Procedural safety was also similar, with low rates of severe complications and no difference in peri-procedural adverse events.
However, major stent malapposition occurred significantly less frequently in the IVL group compared with the RA group (57.8% vs 80.2%; p = 0.002). Calcified nodules were present in nearly half of the study population and appeared associated with higher rates of malapposition.
At 12-month follow-up, target lesion failure rates were low and similar between groups (1.2% vs 2.4%; p = 0.61), although the study was not powered to detect differences in clinical events.
Critical reading and the relevance for clinical practice:
The ICARE trial provides one of the most robust randomised comparisons between IVL and RA. Overall, one of the key take-home messages of the trial is that meticulous intracoronary imaging guidance, lesion preparation, and stent optimisation may have greater impact on procedural success than the specific calcium modification device itself, with nearly 80% of patients achieving an MSA above 4.5 mm2.
The significantly lower rate of major malapposition observed with IVL represents one of the most intriguing findings of the study. Mechanistically, RA may be affected by wire bias leading to heterogeneous plaque modification, particularly in eccentric or nodular calcification, whereas IVL enables a more homogeneous circumferential calcium fracture with deeper energy penetration. Nevertheless, the absolute rates of malapposition remained remarkably high in both groups, and no corresponding difference in clinical outcomes was observed at 12 months. Therefore, the clinical relevance of these imaging findings remains uncertain and requires longer-term follow-up.
Importantly, despite demonstrating the non-inferiority of IVL compared with RA in balloon-crossable calcified lesions, these findings should not be generalised to all calcified PCI scenarios. ICARE enrolled a highly selected population limited to lesions crossable with a 2.0 mm balloon and excluded left main disease, very long lesions, and uncrossable stenoses, which likely represent the clinical settings where atherectomy retains its greatest value.
Therefore, ICARE does not establish a definitive superiority of IVL over RA, but rather supports the concept that both technologies should be considered complementary tools within contemporary calcium modification strategies. While IVL may often be favored because of its ease of use and favorable safety profile, RA remains indispensable in highly resistant, uncrossable, or complex calcified lesions.
Find out more in this unmissable Twitter discussion
The ICARE OFDI trial simultaneous publication at #EuroPCR 2026@HontonB and @mirvatalasnag walk us through the key findings from this randomised trial comparing IVL- and RA-based strategies for calcified plaque preparation during #PCI.
— EuroIntervention (@EuroInterventio) May 21, 2026
Read the full article:... pic.twitter.com/4p7WTlybAJ


No comments yet!