05 Mar 2026
Interdisciplinary therapeutic strategy in a low-risk patient with aortic stenosis and preserved life expectancy
A 71-year-old low-risk patient with symptomatic severe aortic stenosis and preserved ventricular function presents with progressive dyspnoea and chest pain. With long life expectancy, the choice of treatment demands careful interdisciplinary planning. How would you treat?
Authors




- 71-year-old male patient
- Referred for evaluation of progressive dyspnea on exertion (NYHA II-III) and chest pain
Cardiovascular risk factors | Clinical presentation | Lifestyle |
Arterial hypertension | Height: 185 cm | Retired |
Elevated lipids | Weight: 105 kg | Active at home |
Former smoker | BMI: 30.7 kg/m2 |
Case planning: Echo
- p-max / mean: 82 / 42 mmHg
- v-max: 3.9 m/s
- EOA: 0.8 cm2
- LV-EF 64 %, preserved RV function
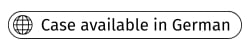
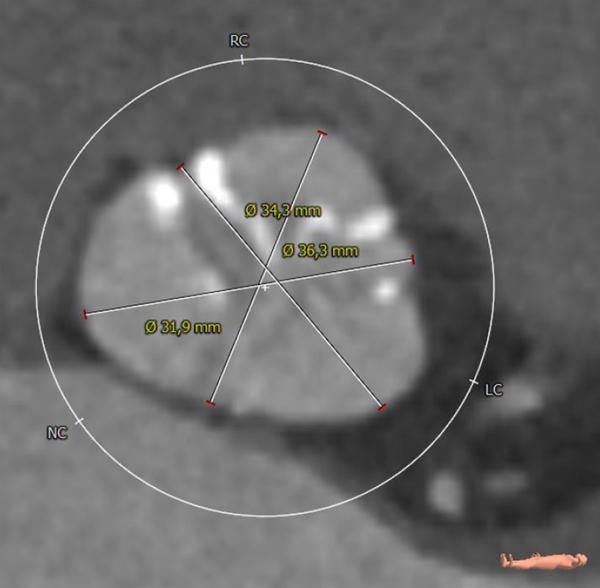
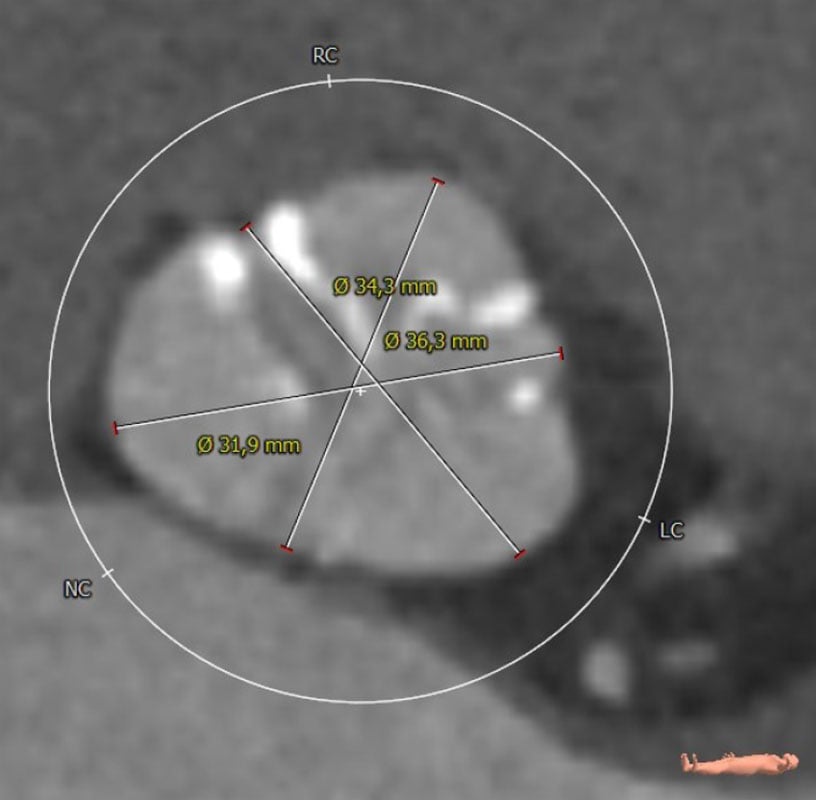
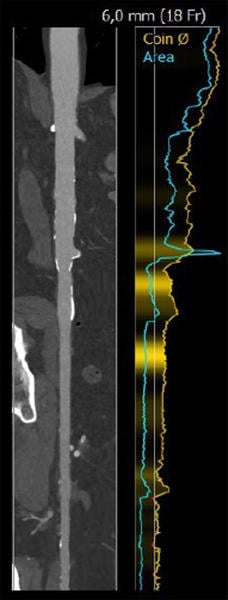
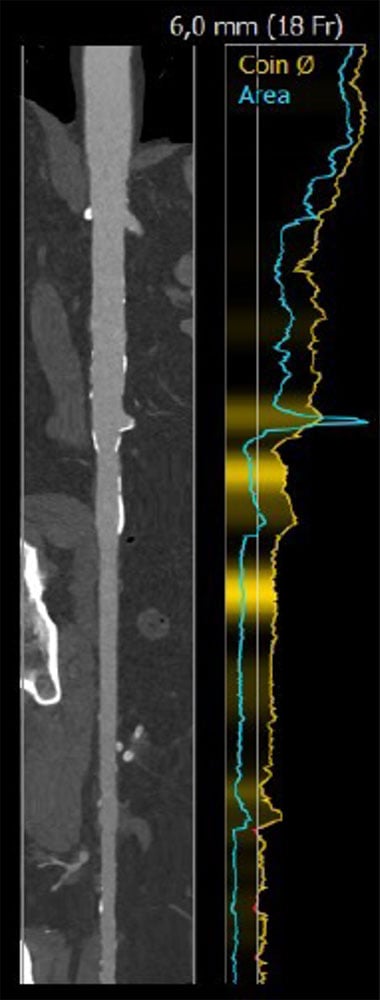
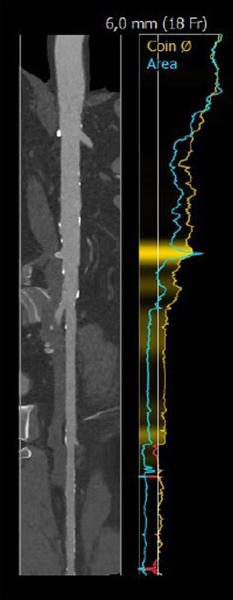
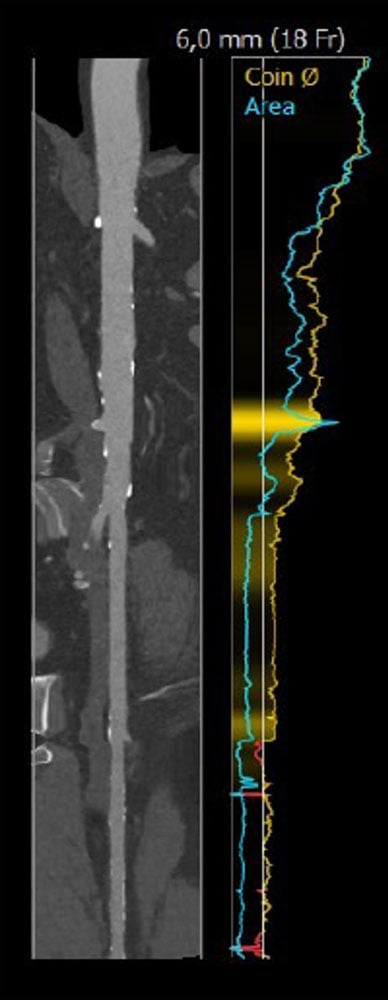
Case planning: CT

Annulus: 29.6 cm
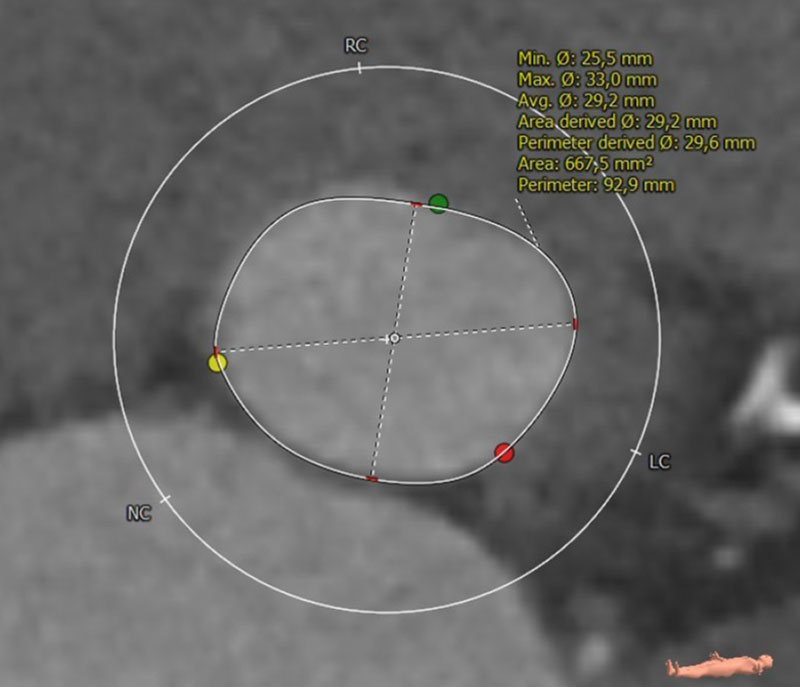

LVOT: 32.2 cm
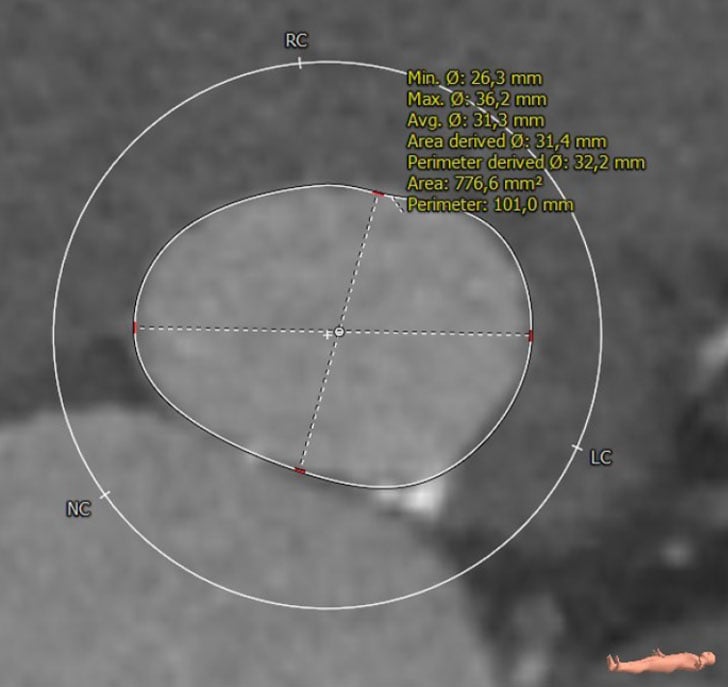
Moderate Ca2+, tricuspid
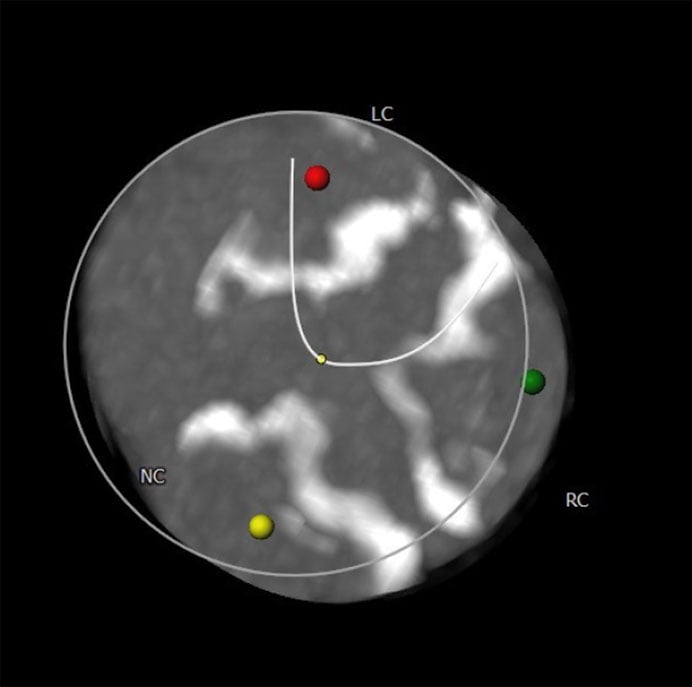
Sinus of Valsalva

LCA: 15.9 mm
RCA: 22.2 mm

Right
Left


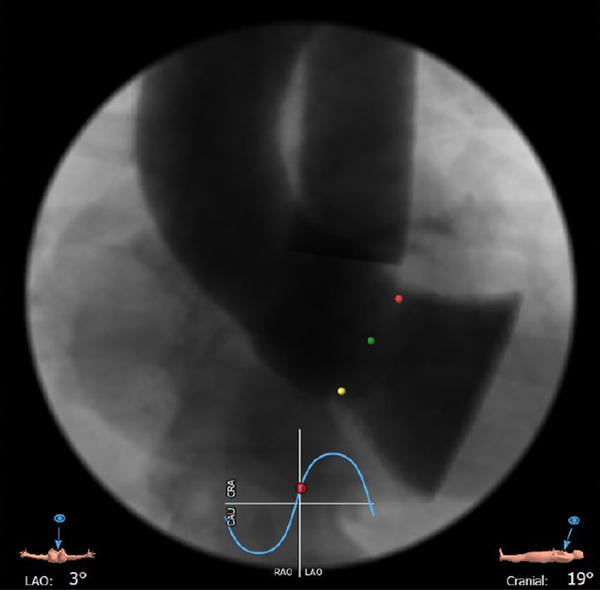
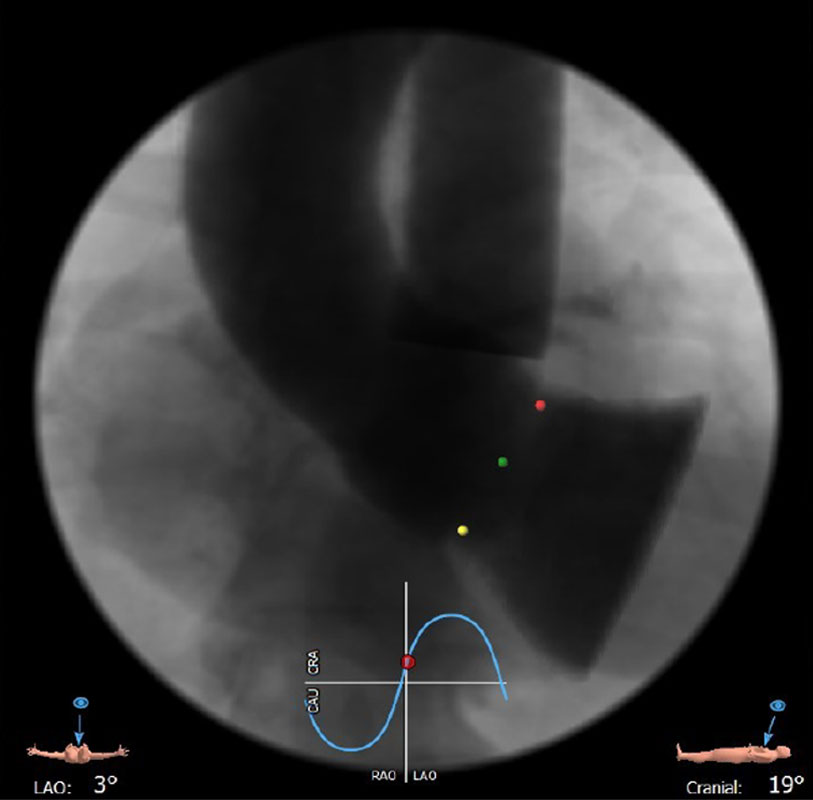
LAO 3° - cranial 19°
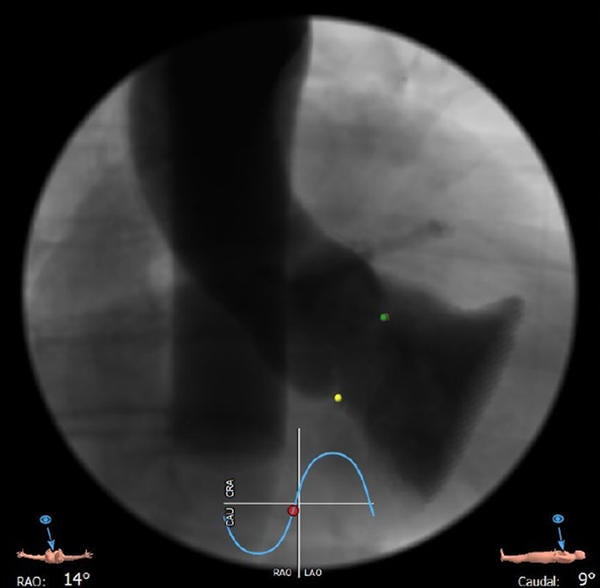
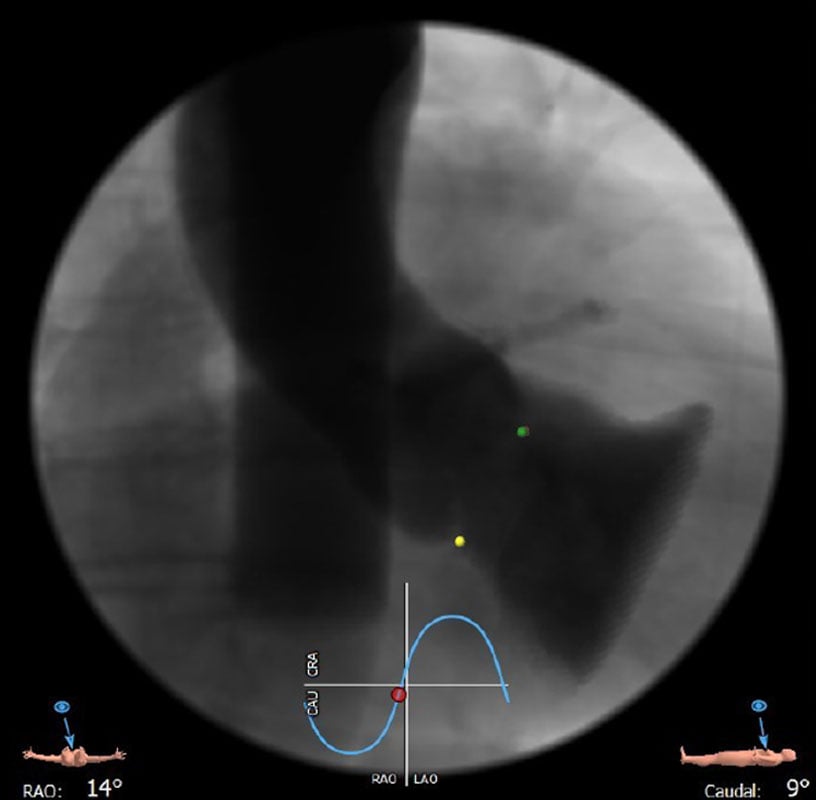
RAO 14° - caudal 9°
Learning objectives
- Learn why and how cardiac CT is playing an increasingly important role in the evaluation of patients with severe aortic stenosis (e.g., calcium score, coronary evaluation)
- Learn what the rationale is to offer patients with asymptomatic severe aortic stenosis AVR
- Understand which aspects can be important in the selection of the index valve how this can drive lifetime management
Disclosure
Dr. Conradi reports the following disclosures:
- Advisory Board Member for Medtronic, Abbott, and JenaValve
- Consultant for Edwards Lifesciences, Boston Scientific, Venus Medtech, MicroPort, MicroInterventions, Neovasc, Pi-Cardia, 4C Medical, and Smartcanula SARL
1 comment
Only objection to requirement of team approach. In AI era how relevant is team approach to decide for indication for TABR vs SAVR. Low risk is easy to diagnose and high risk is risky to do. What is actual use of team approach?