Gore Cardioform ASD occluder implantation for late progression of TR after Triclip
Supported by the EuroIntervention Journal
Late progression of TR following T-TEER is not uncommon and may be challenging to treat due to anatomical and technical limitations. This is the 1st report of Gore Cardioform ASD Occluder implantation to treat recurrent severe TR after T-TEER.
Authors
Thomas Attumalil1, Alex Patrascu1, Amr Gamal1, Yazeed Almalki1, Geraldine Ong1, Sami Alnasser1, Neil P. Fam1
Case summary
A 76-year-old man presented with progressive NYHA III dyspnea, fatigue and edema four years after transcatheter tricuspid edge-to-edge repair (T-TEER). He had been previously treated with two TriClip XT devices (Abbott, Santa Clara, CA) placed between the anteroseptal and posteroseptal leaflets using a clover technique, which initially reduced tricuspid regurgitation (TR) from massive to moderate, with favourable clinical improvement.
The transesophageal echocardiogram (TEE) demonstrated severe TR between the two clips with a central coaptation gap (Figure 1A; Moving image 1).
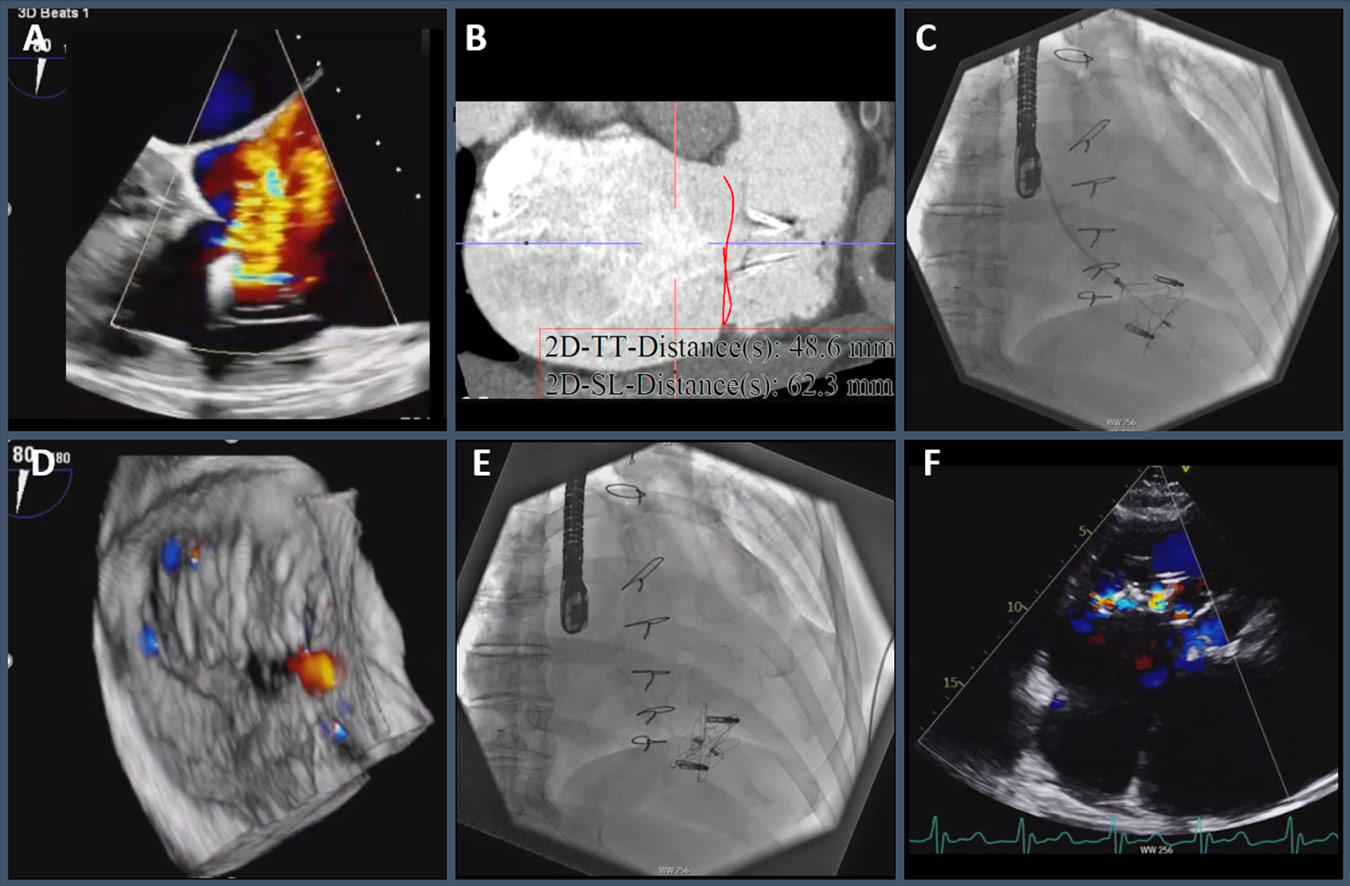
Figure 1. A: 3D echo showing severe TR jet between the two clips. B: CT imaging. C: Fluoroscopy of the 44mm GORE Cardioform ASD occluder implantation. D: 3D echo with mild TR post implantation. E: Fluoroscopy post implantation. F. Echo at 3 months with trace TR.
There was no single leaflet device attachment or suitable targets for redo TEER. EROA of 97 mm2, Reg Vol 79 mL/beat and systolic flow reversal in the hepatic vein were consistent with torrential TR. CT imaging demonstrated tricuspid annular area of 27.5 cm² with perimeter-derived diameter of 60 mm (Figure 1B). The late progression of TR was attributed to ongoing annular dilation secondary to chronic atrial fibrillation. Past history included mitral valve replacement with Maze procedure and previous stroke. TRI-SCORE was 4/12 with STS score of 4.3%. The patient was unsuitable for redo surgery and the intact tissue bridge precluded TTVR. After heart team review, he was accepted for implantation of a Gore Cardioform ASD Occluder (Gore, Flagstaff, AZ) between the clips.
A transjugular approach was chosen to provide a more coaxial approach to the tricuspid valve. The Gore Cardioform ASD Occluder is a highly conformable nitinol device with ePTFE covering which provides immediate seal of the regurgitant orifice. Device sizing was based on CT annular diameter of 60 mm with gap between the clips of 24 mm (a 44 mm Gore occluder has ASD treatment range of 23–30 mm). Given massive annular dilatation, the residual tricuspid annular area after device implantation was predicted to be 15.2 cm², thereby avoiding tricuspid stenosis.
A 14F sheath was placed in the right internal jugular vein with preclosure. An Agilis deflectable catheter (Abbott, Santa Clara, CA) and balloon wedge catheter were used to navigate between the clips, ensuring a chord-free path into the pulmonary artery (Moving image 2).
After exchanging for the delivery sheath, a 44mm Gore Cardioform ASD occluder was implanted with stable position after tug test, with TR reduction from torrential to mild and mean gradient of 1 mmHg (Figure 1C-E; Moving image 3, 4).
The patient was discharged home the following day with mild TR confirmed on transthoracic echo. At 3 month follow-up, he reported improvement in symptoms to NYHA class I with resolution of edema allowing reduction of diuretics. Echo showed trace TR with a well-seated occluder centrally between the 2 Triclips, mean gradient of 1 mm Hg (Figure 1F; Moving image 5).
Late progression of TR following T-TEER is not uncommon and may be challenging to treat due to anatomical and technical limitations (1, 2). This is the 1st report of Gore Cardioform ASD Occluder implantation to treat recurrent severe TR after T-TEER.
This method may be particularly advantageous in cases where the clover technique has been used, as the clips and tricuspid annulus provide a stable dock for the occluder.
Further studies are needed to evaluate the long-term safety and effectiveness of this novel approach.
References
- von Bardeleben RS, Lurz P, Sorajja P, Ruf T, Hausleiter J, Sitges M, Da Rocha E Silva J, Näbauer M, Weber M, Tang GHL, Heitkemper M, Ying SW, Trochu JN, Kar S, Hahn RT, Nickenig G. Two-Year Outcomes for Tricuspid Repair With a Transcatheter Edge-to-Edge Valve Repair From the Transatlantic TRILUMINATE Trial. Circ Cardiovasc Interv. 2023;16:e012888.
- Attumalil T, Alnasser S, Bisleri G, Ong G, Fam NP. Use of a Septal Occluder to Treat Recurrent Tricuspid Regurgitation After TriClip. JACC Cardiovasc Interv. 2024:S1936-8798.
Affiliations
- Structural Heart Program, St. Michael’s Hospital, University of Toronto, Toronto, Ontario, Canada
Conflicts of interest
Dr. Fam is a consultant to Edwards Lifesciences, Abbott, Cardiovalve, Medtronic, Tricares and inQB8.

No comments yet!