How to choose a snare and how to create a snare in complex PCI scenarios
A problem-solving step by step tutorial
Complex percutaneous coronary intervention (PCI) procedures are dramatically increasing in daily practice. Calcified coronary artery lesions and hostile cardiac anatomy may increase the risk of device dislodgment and/or malposition. In such situations, the use of a snare catheter is pivotal to retrieve and/or reposition the device.
Frequency of the problem:
Expert level:
Summary
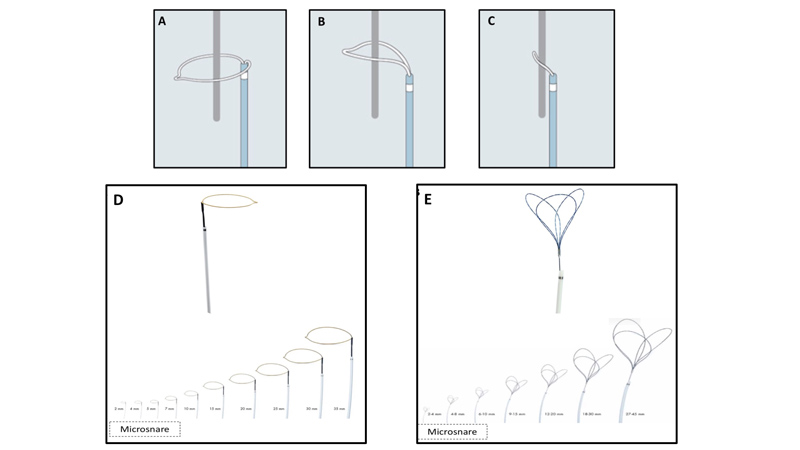
A snare is an endovascular device that consists of one or more radiopaque loops of wire inserted in a catheter, which, when extended, flower out, and, when withdrawn into the catheter, collapse. Its main function is to capture, within the extended loop/loops, any lost or malpositioned devices, with the final aim to retrieve and/or reposition them once its loop/loops are collapsed (Figure 1. A-C).
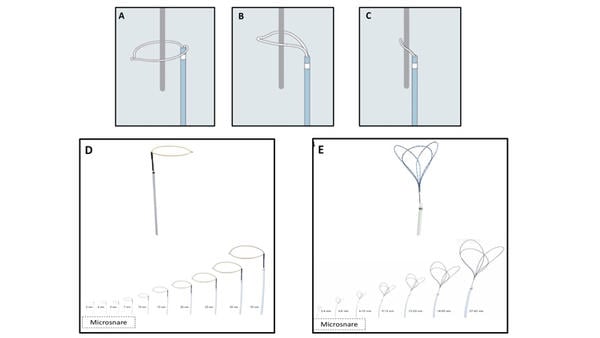
Figure 1 - How a snare works (A-C). A) Snare catheter in the extended configuration (flowered out); B) Once the capturable body is inside the loop, the snare is tightened; C) The foreigner body is secured by the snare and is ready to be retrieved. Different types of snare (with different dimensions) (D-E). D) Single-loop snare; E) Multi-loops snare.
Once vascular access is obtained, the snare is usually inserted through a guiding catheter and placed in proximity to the capturable device.
There are several scenarios in which snare is useful, in particular in the retrieval of a lost device e.g dislodged coronary stent, broken coronary wire, etc.
Many types of snare are available. They vary according to different characteristics: the size of the catheter, its length, and the number and working diameter of its loops. Based on the numbers, snaring systems can be classified into single configurations (e.g Amplatz Goose Neck, Medtronic, or One Snare, Endovascular snare), or multiple overlapping loop configurations (e.g. En Snare, Endovascular snare). Both configurations are available in several different working loop diameters, ranging from a few millimeters (2 to 7 mm, also called microsnare) to some centimeters (up to 35-45 mm) (Figure 1. D-E).
The Problem
The choice of snare type and size largely depends on the type and location of the embolized devices, and the planned retrieval technique.
Although capturing a small device, or one of its small components, may be feasible with a small-diameter loop snare, it appears challenging to succeed if the embolized device is not over a wire, or if its coaxiality with the snare is difficult to achieve. On the contrary, if the purpose is to encircle the entire device, a large snare is required.
On the other hand, the localization of the capturable device, in terms of vessel or cardiac dimensions, is pivotal to safely choose the size of the snare and to avoid traumatic lesions.
The most frequent scenarios in which a snare is useful are depicted below.
Retrieval of a lost coronary stent
This is a potential scenario encountered in the context of PCI for calcified coronary artery disease1. In order to select the proper technique and size, two key aspects should be evaluated:
- Localization of the dislodged stent (inside or outside the coronary vessel)
- Persistence of the dislodged stent on the coronary wire (“total stent loss but guidewire in situ” or “total stent and guidewire loss”)
In general, snaring a lost stent is easier in case of proximal dislodgement in the coronary tree. It is therefore recommended that the free end of the stent be carefully located under fluoroscopy.
The persistence of the stent on the wire (“guidewire in situ”) makes it possible to apply a technique based on the use of microsnare, to reduce the risk of coronary vessel damage (Figure 2. A-D and Video 1)2.
The microsnare is loaded onto the 'in situ' guidewire and advanced close to the lost stent until a perpendicular position is reached (Figure 2. A). Before securing the dislodged stent, the operator must ensure that the snare has correctly encircled the stent (Figure 2.B). The exchange catheter is then advanced and the embolised stent bends as the snare is engaged. To avoid potential crushing of the stent, it is recommended that the stent is wrapped around the proximal segment. When the stent is secured by the snare, the whole assembly is pulled back and extracted (Figure 2. C-D).
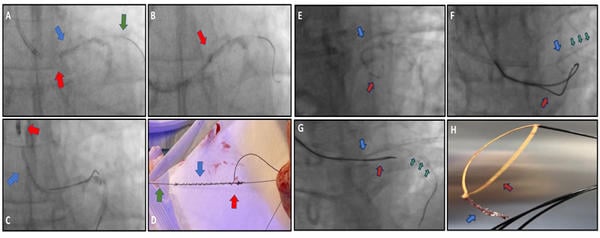
Figure 2 – Snaring a total stent loss but with guidewire in situ (A-D). A) A microsnare (red arrow) is advanced over the guidewire (green arrow) in situ reaching the dislodged stent (blue arrow) in a perpendicular position; B) The proximal part of the dislodged stent is secured by the tightened loop (red arrow); C and D) Retrieval of the entire system.
Snaring a total stent loss without guidewire in situ (E-H). E) Unsuccessful snaring attempt with a microsnare (red arrow) of the prolapsing kinked stent (blue arrow) across left main, after guidewire loss; F) After vessel securing with guidewire (green arrows), a further attempt was perfomed using a larger (30 mm) single-loop snare (red arrow), inserted from the same guiding catheter. The attempt was unsuccessful due to the improper co-axiality between the snare and the dislodged stent; G-H) The use of the same large single-loop snare from a contralateral access, in association with a second guidewire positioning in the coronary artery to stabilize the system, allowed a proper alignment and a successful retrieval.
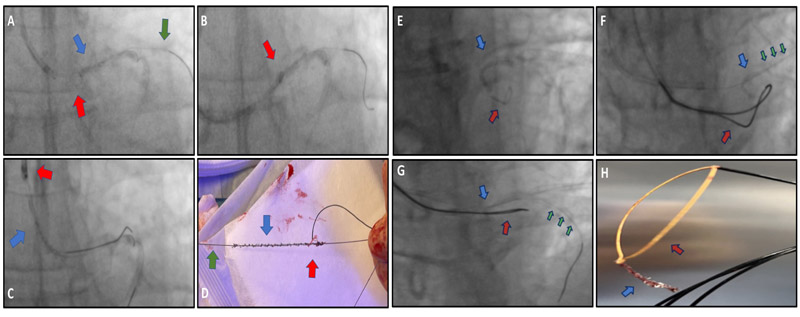
This simple technique is not replicable in case of both total stent and guidewire loss (Figure 2. E-H and Video 2). In this scenario, it is important to understand whether the stent partially protrudes from the coronary tree, which opens up the possibility of using a larger loop snare (Figure 2. E-F). The first step is to secure the coronary vessel with an additional guidewire. The most crucial phase of recovery is obtaining proper coaxiality between the snare and the dislodged stent. If the stent is partially protruding from the left main, insertion of a second guiding catheter with a second guidewire (to stabilize the system) through a contralateral vascular access may allow optimal alignment of the snare and the stent (Figure 2. G-H). Once the operator is confident that the snare has properly encircled the lost device, the retrieval steps are the same as those previously described3.
Principal idea
Snaring is not often used in daily practice but, as seen before, it can be an important tool. Due to its infrequent use, desired dimensions of snare devices in the cathlab are limited and not always suitable for the specific situation. It may be of interest to know that a “homemade” snare can be created in few steps [also called KAM-snare7,8]. The homemade snare is size-adjustable and can be applied to catch different foreign bodies.
Material needed
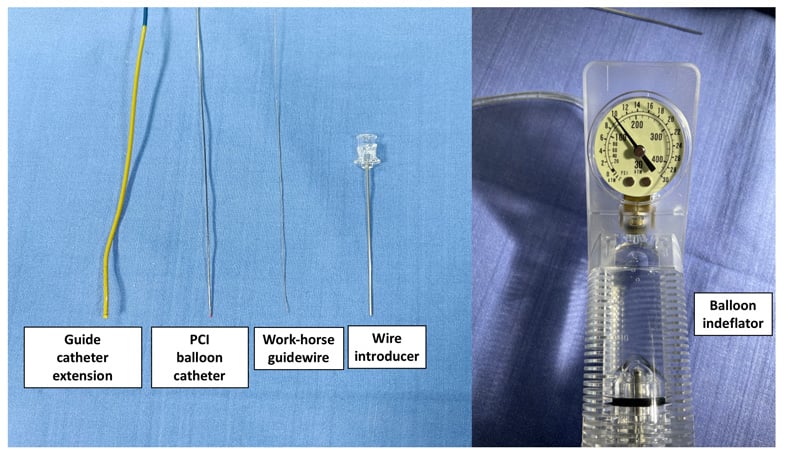
The material used for a homemade snare is depicted in Figure 3 and consists of:
- A conventional (workhorse) 0.014” guidewire
- A 2.0 mm semi-compliant balloon catheter
- A 6 Fr guide catheter extension (GCE)
- A balloon indeflator
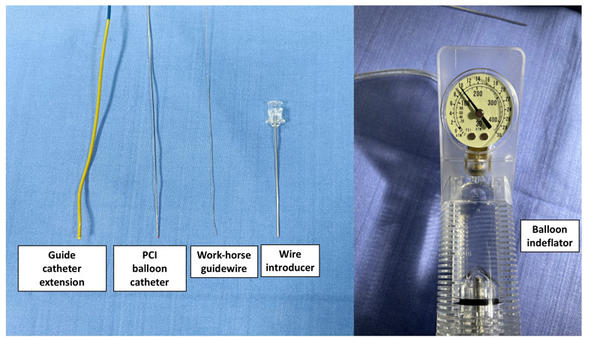
Figure 3 – Material needed to create a homemade snare.
Method step-by-step
Step 1
The 0.014” guidewire is inserted into the wire lumen of the 2.0 mm semi-compliant balloon and advanced until it protrudes 20-30 mm from the balloon tip.
Step 2
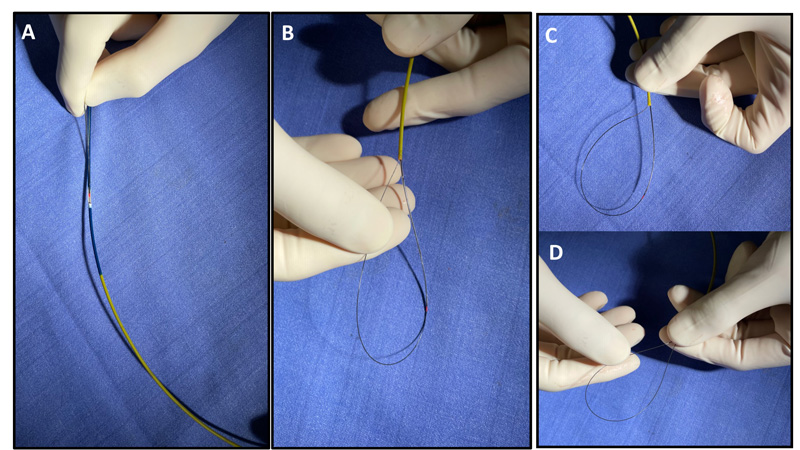
The guidewire tip is folded back towards the balloon in a loop fashion, then the whole system is inserted in the 6 Fr GCE (Figure 4. A) and advanced up to 10 mm from the tip (Figure 4. B-C)
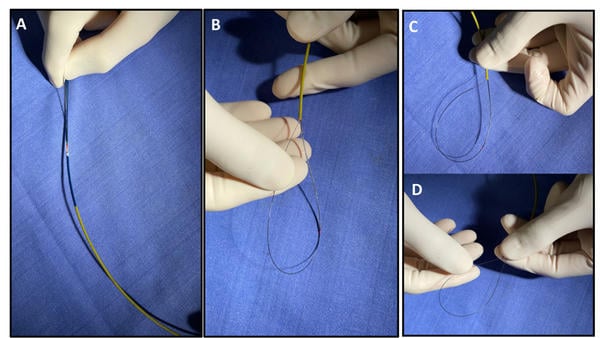
Figure 4 – Step by step homemade snare construction. A) A conventional guidewire and a 2.0 mm balloon are inserted into a 6 Fr guide catheter extension (GCE); B) the proximal end (10-20 mm) of the guidewire is looped inside the (GCE) and trapped by the inflated balloon; C-D) Advancing the distal end of the guide wire is possible to modulate the dimension of the homemade snare’s loop.
Step 3
The folded guidewire is trapped by balloon inflation (usually 8-12 atm) into the GCE.
Step 4
Advancement of the guidewire shaft will produce a size-adjustable snare loop (Figure 4.D and Video 3)
Points of specific attention
- For setting up the homemade snare, various PCI balloons are suitable, as long as their size do not exceed the inner diameter of the GCE (However, a 2.0 mm semi-compliant balloon is recommended).
- To avoid vessel damage, selection of a soft guidewire is preferable. Moreover, using the floppy part at the tip of the guidewire further improves safety.
- In rare cases, the wire lumen of the balloon collapses during inflation, making wire movement impossible. For this reason, an initial functional test of the constructed snare system built outside the body is suggested.
- To adjust the size of the snare loop, simply pulled the snare wire backwards and push it forward (Video 3).
- A case of homemade snare used to retrieve a lost wire in the left subclavian artery is shown in Video 4.
A word from the reviewer - Alexander Völz

Stent loss or ruptured coronary guidewires are a rare but dreaded complication potentially associated with negative outcomes. The three main management options are percutaneous removal, surgery, and in certain scenarios also a conservative treatment. In most cases interventional retrieval is necessary.
Considering the increasing complexity of coronary interventions in our daily practice every interventional cardiologist should be familiar with the available „percutaneous extraction-options“. A homemade snare can be an effective and valid bailout-option. Especially the adjustability to different sizes is advantageous. Due to the infrequence of the problem though homemade snares could also be malfunctioning if not „built“ correctly. Snaring with a dedicated device is a safe, easy and effective approach. I would strongly encourage to provide for at least one type of dedicated snaring-device in every cathlab.
References
- Giannini F, Candilio L, Mitomo S, et al. A practical approach to the management of complications during percutaneous coronary intervention. JACC Cardiovasc Interven. 2018;11(18):1797‐1810. https://www.pcronline.com/Cases-resources-images/Complications/Implant-loss/Stent-loss
- Restivo A, Stanzione A, Maffeo D, Buono A. Ping-pong snaring of a totally dislodged stent across left main ostium: "All is not lost". Catheter Cardiovasc Interv. 2023 Sep 13. doi: 10.1002/ccd.30833. Epub ahead of print. PMID: 37702150.
- Buono A, Medda M, Cesna S, Davidavicius G, Casilli F, Bande M, Pellicano M, Tespili M, Ielasi A. Snaring the Transcatheter Heart Valve Delivery System During Aortic Valve Replacement: When and Why. Cardiovasc Revasc Med. 2021 Jul;28S:81-84. doi: 10.1016/j.carrev.2021.02.018. Epub 2021 Feb 16. PMID: 33674218.
- Mashayekhi K, Valuckiene Z, Neuser H, Akin I, Reifart N, Toma A, Neumann FJ, Behnes M. Wire externalisation techniques for retrograde percutaneous coronary interventions of chronic total occlusions. EuroIntervention. 2017 Dec 8;13(12):e1489-e1490. doi: 10.4244/EIJ-D-16-00009. PMID: 29208580
- Yokoi K, Sumitsuji S, Kaneda H, Siegrist PT, Okayama K, Ide S, Mizote I, Kumada M, Kuroda T, Tachibana K, Sakata Y, Nanto S. A novel homemade snare, safe, economical and size-adjustable. EuroIntervention. 2015 Mar;10(11):1307-10. doi: 10.4244/EIJV10I11A220. PMID: 24642569
View how to enhance device trackability in structural interventions
Authors





No comments yet!