05 Nov 2025
A simple maneuver to track the wire during a transseptal mitral valve-in-valve procedure
A problem-solving step-by-step tutorial
Advancing a transcatheter heart valve through the septostomy can be tricky, with the wire sometimes prolapsing into the left atrium.
This step-by-step tutorial demonstrates a simple yet effective maneuver that allows smooth, controlled navigation from the right atrium to the mitral position, ensuring precise valve deployment.
Frequency of the problem:
Expert level:
Summary
During transseptal mitral valve-in-valve procedures using a balloon-expandable system (e.g. Edwards Sapien), the delivery catheter is oriented 180° downward (the E-logo facing down), in contrast to the standard TAVI procedure in the aortic position.
As a result, gentle clockwise rotation of the delivery catheter combined with additional flexion enables a leftward and posteriorly directed advancement. A simple maneuver—clockwise rotation of the balloon-expandable delivery system handle with simultaneous flexion and catheter advancement—allows smooth and controlled navigation from the right atrium into the left atrium through the septostomy.
Returning the catheter to the neutral position then facilitates the advancement of the transcatheter heart valve from the left atrium into the mitral position (toward the left ventricle): see explanations below.
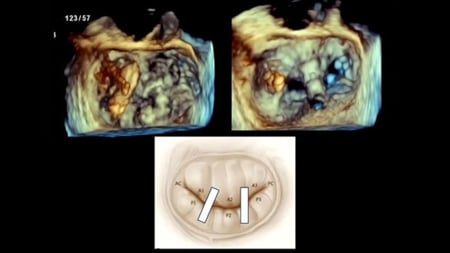
Step-by-step method (Figure 1: a, b and c)
Step 1
Rotate the handle and flexion knob clockwise with the 'E' logo facing downward to help the device more rightward and posteriorly across the interatrial septum (Figure 1a).
Step 2
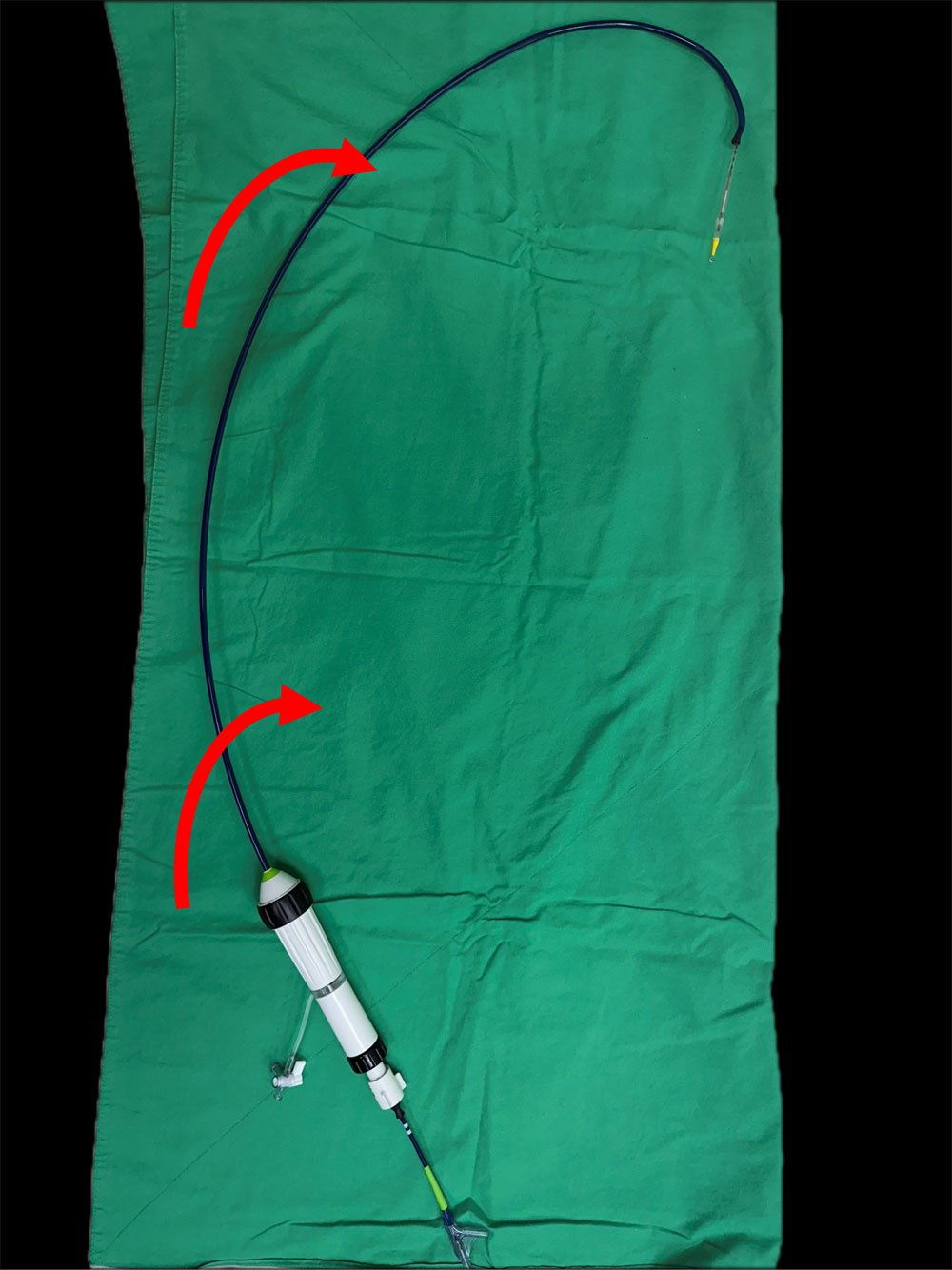
Right atrium into left atrium is posteriorly directed: apply flexion and clockwise rotate the delivery handle (red arrow) (Figure 1b).

Figure 1a

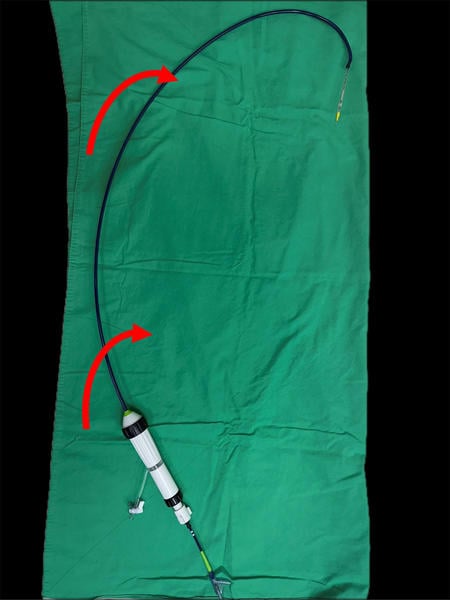
Figure 1b
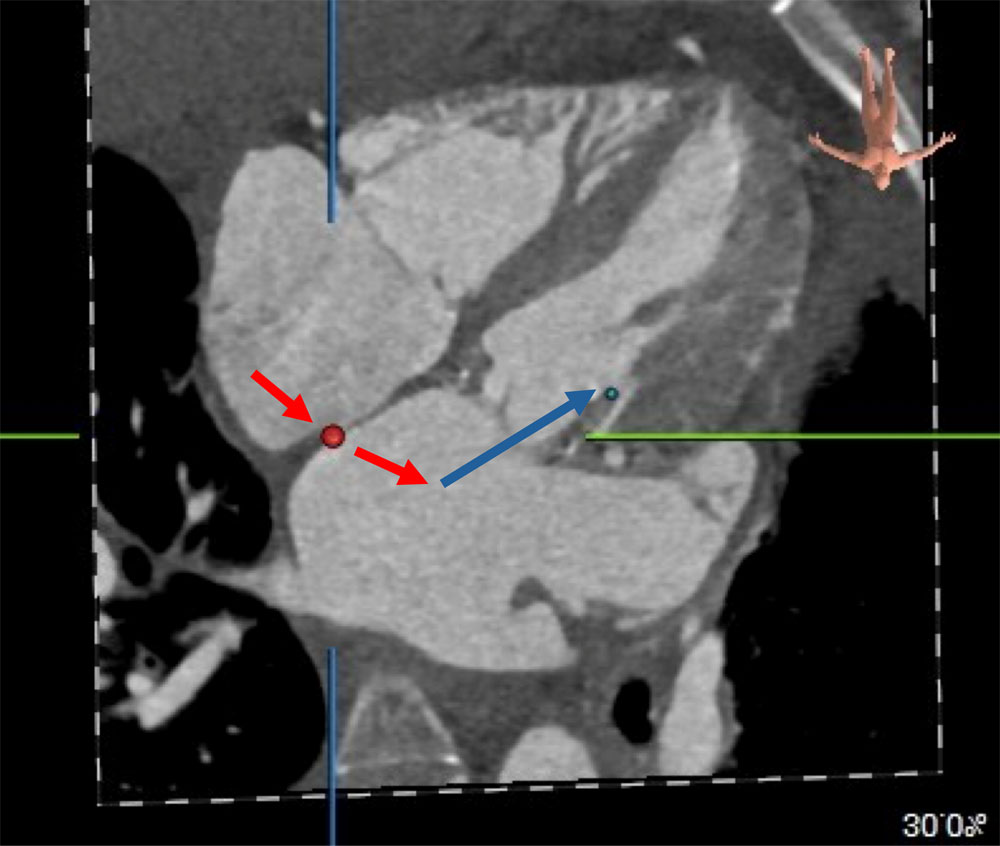
Step 3
Left atrium into mitral position is anteriorly directed: resume neutral position of the delivery handle (blue arrow) (Figure 1c).
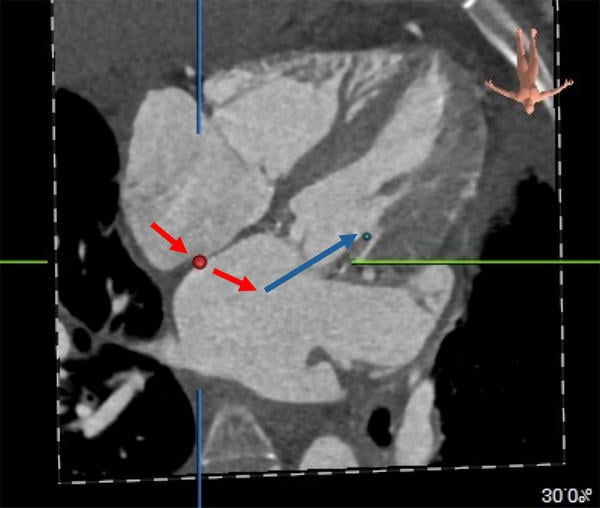
Figure 1c
The problem
During transseptal mitral valve-in-valve procedures, advancing the transcatheter heart valve (THV) through the septostomy can sometimes be challenging, even after adequate balloon dilatation.
In addition, there is a tendency for the wire to prolapse into the left atrium during THV advancement. This difficulty may be attributed to the multiple angulations involved: from the inferior vena cava into the right atrium, from the right atrium into the left atrium (posteriorly directed), and from the left atrium into the left ventricle (anteriorly directed).
Principal idea
A simple gentle clockwise rotation of the delivery catheter while applying flexion node can allow smooth and controlled navigation across the right atrium into the left atrium.
Returning the catheter to the neutral position then facilitates the advancement and accurate positioning of the transcatheter heart valve in the mitral position.
Material needed
None
Step-by-step method (Video 1)
Step 1
Apply gentle clockwise rotation of the delivery catheter while simultaneously flexing and advancing the transcatheter heart valve from the right atrium into the left atrium (through the interatrial septum).
Step 2
Once the transcatheter heart valve is in the left atrium, return the delivery catheter to the neutral position to facilitate further advancement.
Points of specific attention
The operator should rotate the delivery system clockwise with simultaneous flexion and forward advancement. Only gentle and small rotations (equivalent to about 5–10 minutes on a clock face) are sufficient, and care should be taken to avoid over-rotation.
This concept can also be applied to tricuspid valve-in-valve procedures. During advancement of the THV from the right atrium into the right ventricle, gentle counterclockwise rotation of the delivery handle may facilitate anteriorly directed advancement.
N.B. : This article was inspired by the previous one about "Inner curvature technique for the implantation of a balloon-expandable valve".
The invited Expert's opinion

Transseptal transcatheter mitral valve-in-valve implantation of a balloon-expandable valve is an excellent indication for treatment of a degenerated bioprosthesis in patients with an increased surgical risk.
However, advancing the implant catheter through the septum is in some cases a challenging situation. There are different options existing for supporting this maneuver like using a larger ballon for the septostomy, using a stiffer wire (e.g Lunderquist) instead of a regular preshaped wire (e.g. Safari, Confida) or using of an additional safety wire.
The described technique in this article is an other option and very simple to use without the need for any additional material or steps. Crossing the septum with a clockwise rotation and simultaneously flexing of the implant catheter might help and is easy to use. I am very thankful to the authors for sharing this simple technique.
Disclosures
The authors have no conflicts of interest to declare.
Authors





1 comment
fully endorsed