24 Jun 2026
Microsafety: the ipsilateral safety wire technique
Protection wire through superficial femoral artery micropuncture in patients undergoing TAVI: when, how, why
Frequency of the problem:
Expert level:
A practical strategy to improve safety in transfemoral TAVI access
Transfemoral (TF) access remains the preferred route for transcatheter aortic valve implantation (TAVI).
Advances in delivery systems, lower-profile sheaths, computed tomography (CT) based procedural planning and ultrasound-guided puncture have substantially reduced vascular complications. However, challenging iliofemoral anatomy (severe calcification, vessel tortuosity) continues to increase procedural complexity and risk of vascular complications.
We describe a practical approach that aims to improve the safety of TF-TAVI access by combining a ipsilateral safety wire strategy with a micropuncture technique. The goal is to provide a vascular “safety net” while avoiding additional access-related complications.
Challenges in high-risk transfemoral TAVI access
Severe calcification, tortuosity, small vessel calibre, and diffuse may complicate large-bore sheath delivery and vascular closure. Although pre-procedural CT planning helps identify the optimal puncture site, complications such as dissection, perforation, vessel closure, or closure device failure may still occur, especially in patients with advanced peripheral artery disease.
Importantly, certain access site complications, being occlusion or bleeding, can be identified only when main vascular access is supposed to be closed, limiting the access to a quick solution.
Combining micropuncture and ipsilateral safety wire for vascular protection
The micropuncture technique offers several advantages:
- A lower-profile needle (24-gauge versus standard 18-gauge):
- very-small initial vessel puncture
- less trauma to the arterial wall and low risk of additional vascular complication
- The safety wire provides immediate and ‘on-site’ vascular access if complications occur during common femoral artery (CFA) puncture or after access site closure
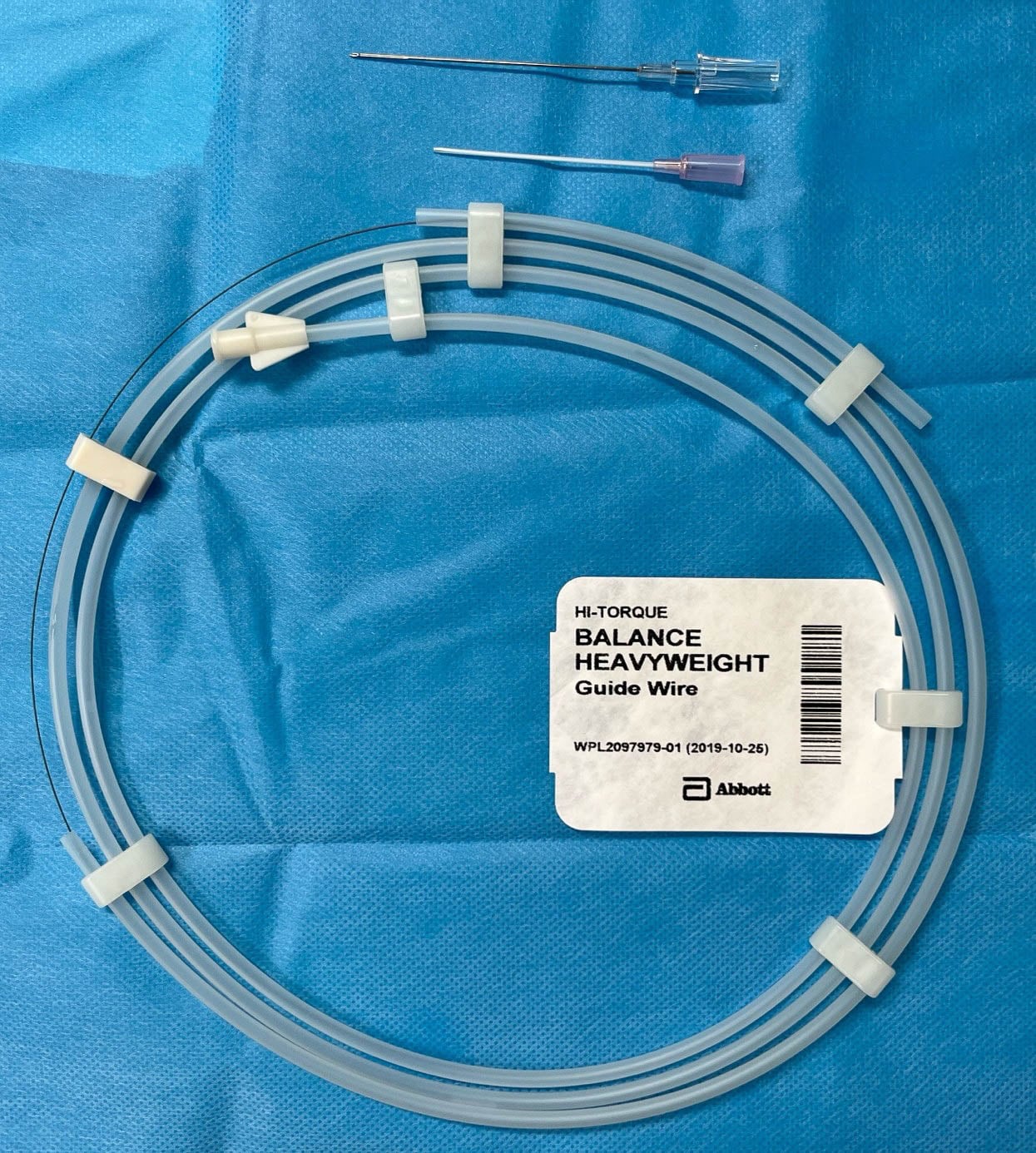
Materials needed
- Ultrasound
- Micropuncture access sets (i.e. radial puncture set):
- lower-profile needle compared to standard introducer kits
- micropuncture sheath
- 0.018-inch coronary guidewire – ideally extra support design

Method step-by-step
Step 1 – Preparation
Prepare the groin and optimise ultrasound imaging. Shape the tip of the 0.018-inch guidewire to facilitate atraumatic advancement.
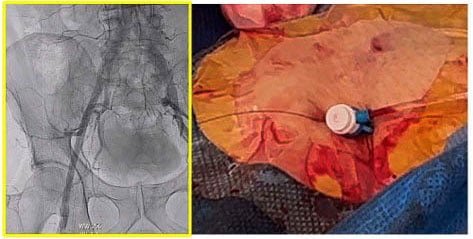
Step 2 – Safety access
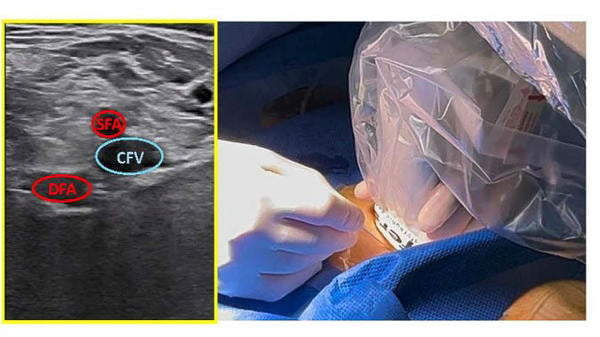
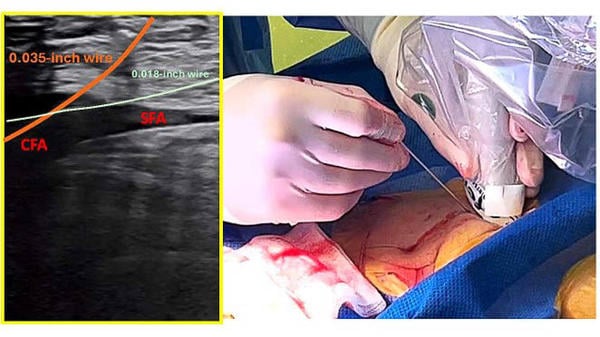
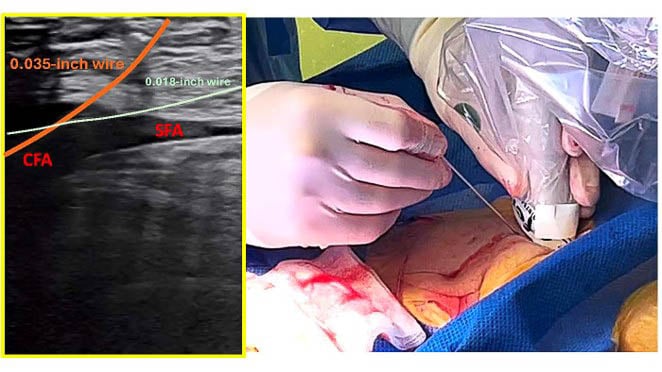
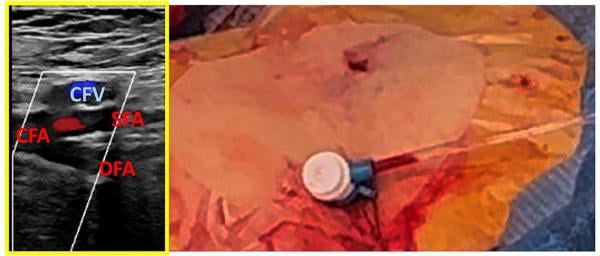
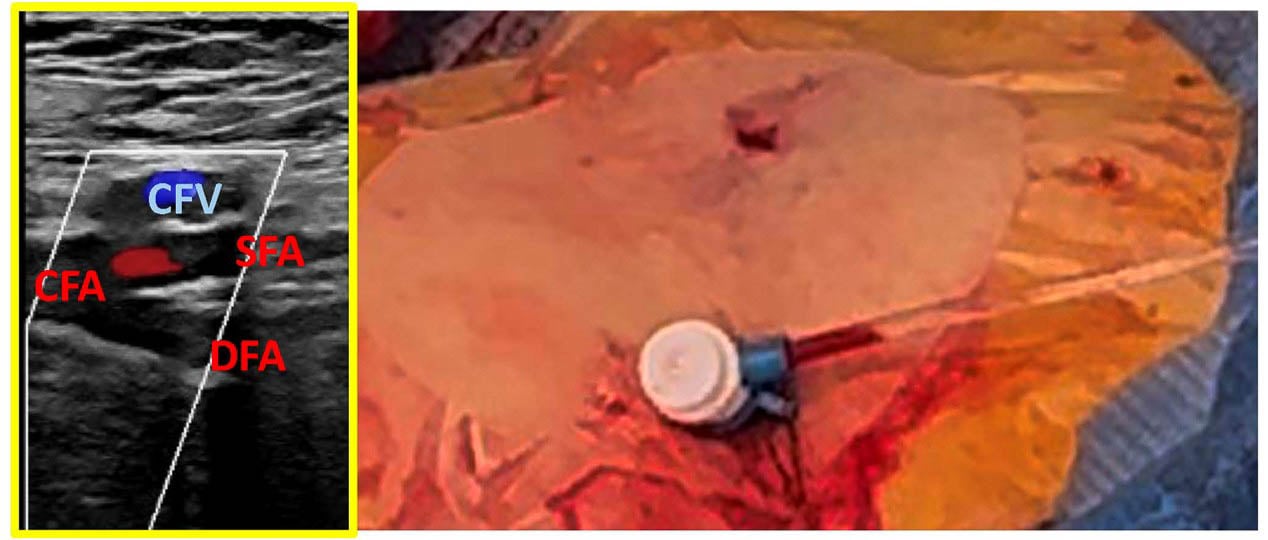
Under ultrasound guidance, puncture the superficial femoral artery (SFA) on the ipsilateral side using the micropuncture set.
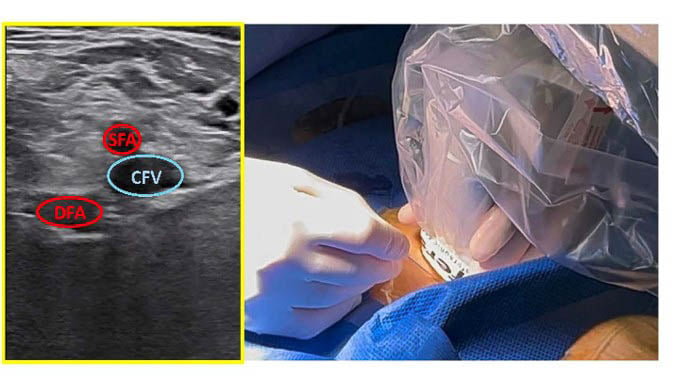
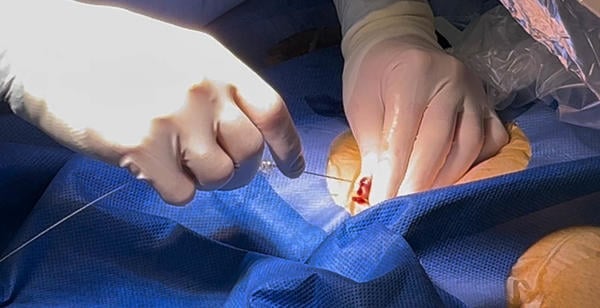
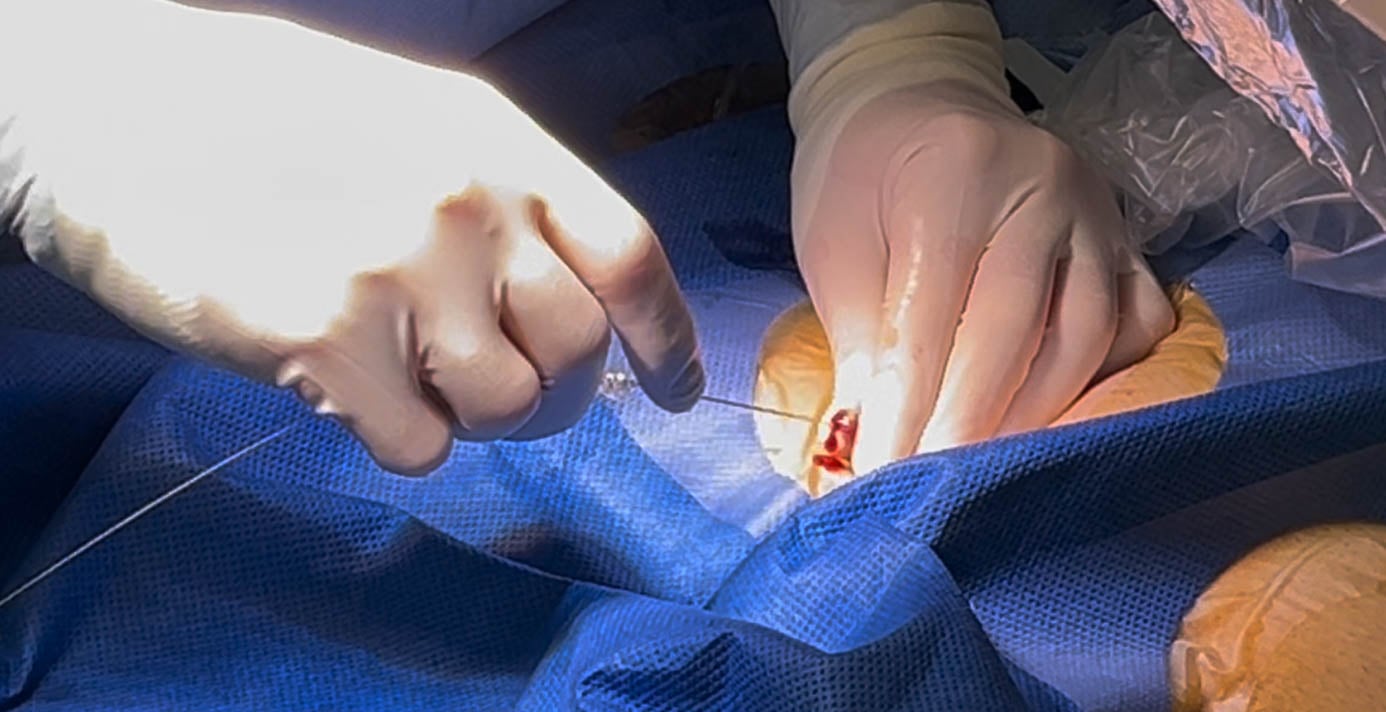
Step 3 – Safety wire placement
Advance the 0.018-inch extra-support coronary guidewire through the micropuncture sheath to establish a safety access route. Remove the micropuncture sheath while maintaining wire position.

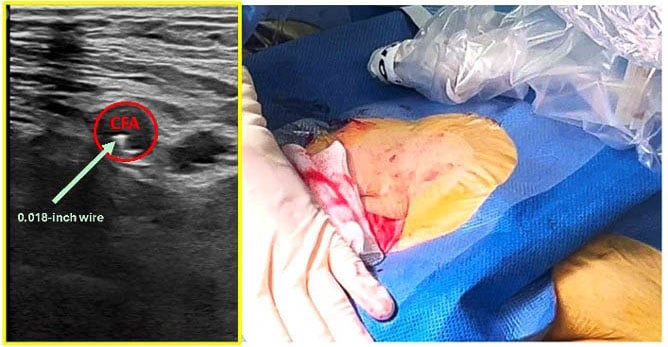
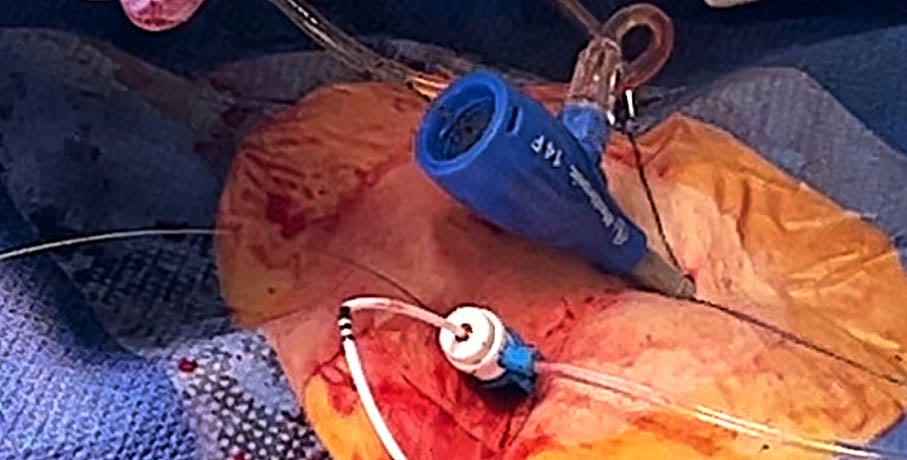
Step 4 – Main femoral access
Using ultrasound guidance, perform puncture of the common femoral artery (CFA) with a standard 18-gauge needle at the pre-planned access site.
Step 5 – TAVI procedure
Proceed with TF-TAVI according to standard practice. The pre-positioned safety wire may be used for bailout solution if vascular complications arise during access site closure.

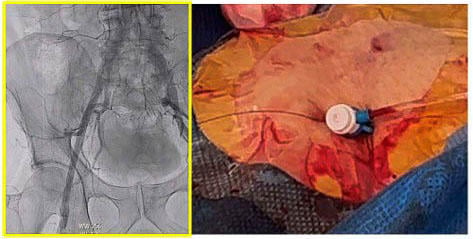
Step 6 – Closure
Remove the large-bore sheath and close the main access site while maintaining safety wire access. Perform a control angiogram. If no vascular complication is identified, remove the safety wire.
Points of specific attention
- Consider ipsilateral safety wire technique in patients with severe femoral calcification or extreme tortuous anatomy, limiting bail-out strategies for vascular complication via secondary radial access or via contralateral femoral access
- Ultrasound guidance remains essential to achieve optimal SFA access for the safety wire and optimal CFA access above the bifurcation and below the inguinal ligament.
- The extra-support 0.018-inch guidewire provides sufficient stability to rapidly advance a sheath, diagnostic catheter, balloon, or covered stent in the event of a vascular complication.
- Adequate distance from the main puncture site allows effective device positioning and treatment.
A word from the reviewer

The concept of maintaining ipsilateral arterial access as a bailout route was previously described by Frerker et al., who demonstrated that a distal ipsilateral access strategy facilitated angiographic assessment and endovascular treatment of vascular complications during TAVI. In their study, the double-access technique reduced contrast use and was associated with fewer major vascular complications and surgical repairs, although minor vascular complications were more frequent and no difference in 30-day mortality was observed (1).
The present micropuncture-based safety wire technique represents an elegant refinement of this concept. By replacing a secondary sheath with a low-profile SFA micropuncture access and a retained 0.018-inch guidewire, operators preserve immediate bailout access while minimizing additional arterial trauma. Simple, inexpensive, and easy to adopt, this technique may be particularly useful in patients with hostile iliofemoral anatomy where rapid bailout options are essential. It reflects a proactive approach to vascular access management, emphasizing preparedness rather than rescue.
Reference
- Frerker C, Schewel D, Kuck KH, Schäfer U. Ipsilateral arterial access for management of vascular complication in transcatheter aortic valve implantation. Catheter Cardiovasc Interv. 2013;81:592–602.
Authors



