PARTNER 2 at 10 years: transcatheter or surgical aortic valve replacement in intermediate-risk aortic stenosis
Selected in JACC by A. Sticchi
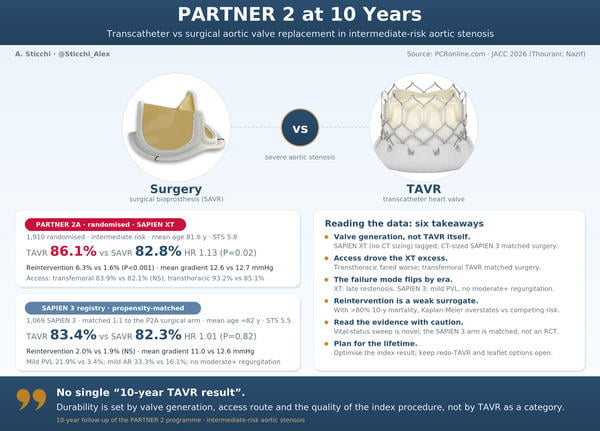
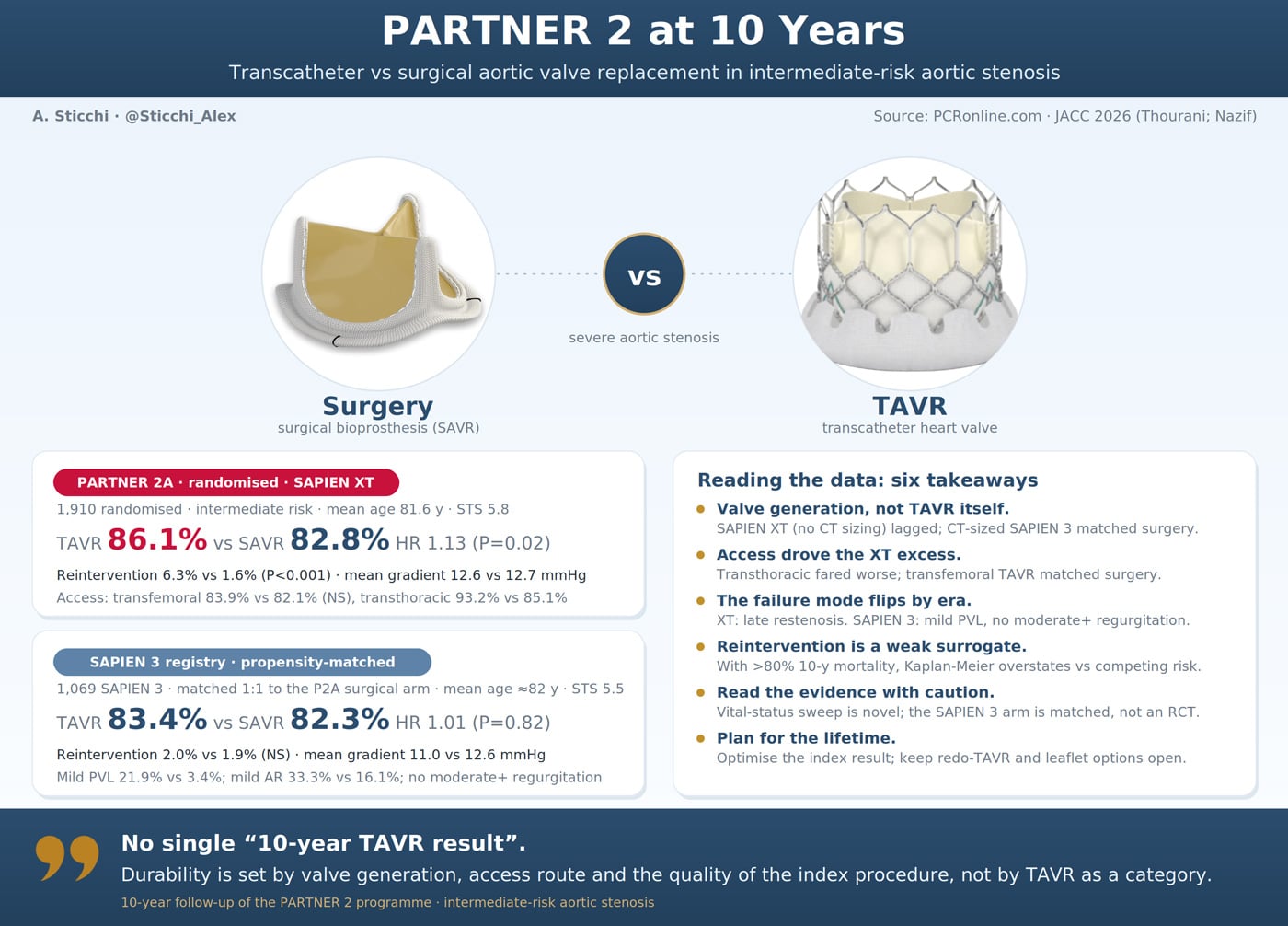
At 10 years, the second-generation SAPIEN XT was associated with lower survival and higher reintervention than surgery in the randomised PARTNER 2A trial, whereas the third-generation SAPIEN 3 matched surgery in a propensity-matched registry comparison. Two analyses, one lesson: long-term outcome is defined by the valve and the index procedure, not by TAVR as a category.
References
Authors
Thourani VH, von Stein P, Mack MJ, Nazif TM, Babaliaros V, Alkhouli M, Fischbein MP, Desai ND, Satler L, Zidar FJ, Kodali SK, Kron IL, Zajarias A, Brinkman W, Kapadia S, Dewey TM, Gössl M, Bodenhamer RM, Ma Y, Cohen DJ, Sharma R, Pibarot P, Hahn RT, Leon MB, Makkar RR; PARTNER 2 Investigators
Reference
J Am Coll Cardiol . 2026 Jun 16;87(23):3309-3321.
Published
16 June 2026
Link
Read the abstractReviewer

My Comment
ORIGINAL PAPERS
- PARTNER 2A (randomised) - Thourani VH, von Stein P, Mack MJ, et al. 10-year randomized outcomes of transcatheter or surgical aortic valve replacement in intermediate-risk aortic stenosis. J Am Coll Cardiol. 2026;87(23):3309-3321.
- PARTNER 2 S3i (registry, propensity-matched) - Nazif TM, Simonato M, Makkar RR, et al. 10-year outcomes of SAPIEN 3 transcatheter aortic valve replacement or surgery in intermediate-risk patients. J Am Coll Cardiol. 2026;87(23):3296-3308.
Why this study – the rationale/objective?
TAVR is an established alternative to surgery across the surgical risk spectrum, and the debate has shifted from short-term safety to long-term durability.
Randomised comparisons have shown TAVR to be non-inferior or superior to surgery at early and mid-term follow-up, but high-quality 10-year comparative data, particularly with contemporary valves, have been lacking.
The 6 to 10-year window is increasingly recognised as the onset of vulnerability for bioprosthetic valve failure, and these data are decisive for lifetime management as TAVR moves toward younger patients.
This JACC package reports the 10-year outcomes of the intermediate-risk PARTNER 2 programme through two complementary analyses, accompanied by three editorials and a methodological Special Communication.
How was it executed? The methodology
Two prospective, multicentre, industry-sponsored studies using identical eligibility criteria and access stratification (transfemoral vs transthoracic) were analysed.
In the first analysis, Thourani et al. report the randomised PARTNER 2A trial: 1,910 intermediate-risk patients enrolled at 57 centres between 2011 and 2013 and randomised 1:1 to TAVR with the second-generation SAPIEN XT or to surgery. CT-based annular sizing was not required and valve sizes were initially limited to 23 and 26 mm.
In the second analysis, Nazif et al. report the PARTNER 2 SAPIEN 3 Intermediate-Risk Registry (P2S3i), which enrolled patients in 2014 with the third-generation SAPIEN 3 (CT-guided sizing, lower-profile delivery, improved sealing skirt). Because SAPIEN 3 was introduced after PARTNER 2A enrolment closed, S3 patients were propensity-matched 1:1 to the PARTNER 2A surgical arm, yielding 783 pairs.
Both trials were originally designed for a 5-year follow-up and extended to 10 years at the request of the FDA, which required patient reconsent at 5 years. To recover mortality data in patients who declined reconsent, the investigators applied vital status sweeps using medical records and publicly available sources. Endpoints were all-cause mortality, aortic valve reintervention, and core-laboratory-adjudicated echocardiography.
What is the main result?
In the randomised PARTNER 2A trial (974 TAVR, 936 surgery; mean age 81.6 years, STS 5.8%), 10-year all-cause mortality was higher after SAPIEN XT TAVR than surgery: 86.1% vs 82.8% (HR 1.13; 95% CI 1.02 to 1.25; P = 0.02).
The excess was concentrated in the transthoracic cohort (93.2% vs 85.1%; P < 0.01), whereas transfemoral TAVR did not differ from surgery (83.9% vs 82.1%; P = 0.27), with a significant access interaction (P = 0.03).
Aortic valve reintervention was about four-fold higher with TAVR (cumulative incidence 6.3% vs 1.6%; P < 0.001). Among the few patients with echocardiography at 10 years, mean gradients were comparable (12.6 vs 12.7 mmHg).
In the propensity-matched SAPIEN 3 registry comparison, outcomes were similar between groups: 10-year all-cause mortality 83.4% vs 82.3% (HR 1.01; 95% CI 0.91 to 1.13; P = 0.82), and competing-risk-adjusted reintervention 2.0% vs 1.9% (P = 0.47). Hemodynamics were stable (mean gradient 11.0 vs 12.6 mmHg), with mild aortic regurgitation and mild paravalvular leak remaining more frequent after TAVR but no moderate or greater total regurgitation.
Critical reading and the relevance for clinical practice
The two analyses appear to point in opposite directions, and the first task is to decide whether the divergence is real. In the randomised PARTNER 2A comparison the second-generation SAPIEN XT carried a higher 10-year all-cause mortality than surgery (86.1% vs 82.8%; HR 1.13, 95% CI 1.02 to 1.25; P = 0.02) and a roughly four-fold excess of aortic valve reintervention (6.3% vs 1.6%; P < 0.001). In the propensity-matched SAPIEN 3 registry the same endpoints were neutral (mortality 83.4% vs 82.3%; HR 1.01, 95% CI 0.91 to 1.13; P = 0.82; reintervention 2.0% vs 1.9%; P = 0.47). The accompanying editorials converge on reading this not as a contradiction but as a generational effect, and I share that interpretation: the comparison is between two different devices, implanted with different sizing and sealing strategies, against the same surgical benchmark. The neutral S3 result does not overturn the XT signal; it dates it.
The most plausible mechanism linking the two papers is paravalvular regurgitation. Moderate or greater PVL was consistently more frequent with the XT and is an established driver of late mortality, whereas the S3 was engineered against this specific failure mode through an outer sealing skirt and mandatory CT sizing. The residual difference remains informative: even with the S3, mild aortic regurgitation and mild PVL were more frequent after TAVR than after surgery, although no moderate or greater total regurgitation was recorded, which indicates that the sealing problem has been reduced rather than abolished. The two valves also failed differently, with restenosis more prominent after the XT and regurgitation predominating after the S3, a divergence that parallels the distinct degeneration phenotypes of surgical bioprostheses and that has direct implications for what surveillance imaging should look for. Taken together, the data support a device-and-procedure explanation for the XT excess rather than an intrinsic late penalty of the transcatheter approach.
Reintervention warrants cautious interpretation in this population. The rates quoted are competing-risk estimates; the unadjusted Kaplan-Meier figures are substantially higher, and the distance between the two shows how strongly competing mortality shapes the endpoint. In a cohort with a mean age of 81.6 years in which more than 80% had died by 10 years, a structurally failing valve frequently never reaches a second procedure, so reintervention underdetects true valve deterioration and is further conditioned by patient selection and by the clinical decision not to reoperate. It is, in consequence, a weak surrogate for durability, as the editorials note. The interpretation is complicated further by the changing feasibility of redo procedures: as redo-TAVR and leaflet-modification techniques that preserve coronary access become routine, the threshold to reintervene is likely to fall, so reintervention rates measured in the future may not be comparable with the historical figures reported here.
The long-term follow-up is methodologically fragile, and the Special Communication by Vemulapalli and colleagues is candid about it. Both trials were designed for 5 years and extended to 10 at the request of the FDA, with reconsent required at 5 years, so reintervention and echocardiographic data were available only in roughly half of survivors. A vital-status sweep, described as novel and not yet validated, raised mortality completeness to about 90% but recorded survival status only, with no information on valve function or cause of death, and it recovered deaths more readily than survivors. Because the initial loss to follow-up differed between arms and the sweep added more deaths to the surgical group, the direction of the residual bias is uncertain rather than necessarily conservative. The constructive proposal that follows, namely to build adequate follow-up duration, prospective consent for data linkage and reusable real-world infrastructure into future device trials, is the practical lesson of these limitations.
Two further signals should be weighted with care. The hemodynamic reassurance rests on a small sample, since 10-year echocardiography was available in only a few dozen survivors per arm; mean gradients were stable (12.6 vs 12.7 mmHg in PARTNER 2A and 11.0 vs 12.6 mmHg in the S3 comparison), but survivorship bias limits what can be inferred about the unmeasured majority. The excess mortality with transthoracic access (93.2% vs 85.1%; P < 0.01) is an exploratory subgroup finding, and patients referred for a transthoracic approach carry the vascular and atherosclerotic burden that precludes transfemoral access in the first place, a profile that may drive outcome independently of the route. The comparison relevant to current practice is the transfemoral subgroup, in which TAVR did not differ from surgery (83.9% vs 82.1%; P = 0.27, with a significant access interaction, P = 0.03), and I would weight this estimate more heavily than the pooled XT result.
The decisive question is whether these findings extend to the younger, lower-risk patients now directed toward TAVR by the 2025 ESC/EACTS guidelines. On this point the intermediate-risk data reassure only partially, because the competing mortality that conceals late valve dysfunction in octogenarians will not protect a 65-year-old with decades of follow-up ahead. The available lower-risk datasets are not concordant: PARTNER 3 at 7 years showed comparable survival, reintervention and bioprosthetic valve failure with the S3, whereas Evolut Low Risk at 6 years showed a higher and diverging reintervention rate, attributed in part to regurgitation and to aggressive post-dilatation. In my view the 10-year read-outs of these two trials, rather than the present intermediate-risk analyses, will be the datasets that settle the durability question for lifetime management. The message that runs consistently through the package is that long-term outcome after TAVR depends less on the modality than on the device generation and the quality of the index result, in particular the residual paravalvular leak, the accuracy of sizing and the preservation of options for future intervention.
Références
- Thourani VH, von Stein P, Mack MJ, et al. 10-year randomized outcomes of transcatheter or surgical aortic valve replacement in intermediate-risk aortic stenosis. J Am Coll Cardiol. 2026;87(23):3309-3321.
- Nazif TM, Simonato M, Makkar RR, et al. 10-year outcomes of SAPIEN 3 transcatheter aortic valve replacement or surgery in intermediate-risk patients. J Am Coll Cardiol. 2026;87(23):3296-3308.
- Capodanno D, Bujak K. TAVR at a decade: long-term data meet a long-standing debate. J Am Coll Cardiol. 2026;87(23):3322-3324.
- Borger MA. TAVR in lower risk patients: innovation meets uncertainty. J Am Coll Cardiol. 2026;87(23):3325-3327.
- Gupta A. TAVR at 10 years: which valve, which patient, which era? J Am Coll Cardiol. 2026;87(23):3328-3329.
- Vemulapalli S, White R, Hickey GL, et al. Here and now to the horizon: meeting the challenge of 10-year follow-up in transcatheter valve trials. J Am Coll Cardiol. 2026;87(23):3330-3334.
- Leon MB, Mack MJ, Pibarot P, et al. Transcatheter or surgical aortic-valve replacement in low-risk patients at 7 years. N Engl J Med. 2026;394:773-783.
- Forrest JK, Yakubov SJ, Deeb GM, et al. Six-year outcomes after transcatheter vs surgical aortic valve replacement in low-risk patients with aortic stenosis. J Am Coll Cardiol. 2026;87(23):3210-3221.

No comments yet!