16 Apr 2026
Valve choice for TAVI: pros and cons for intra- and supraanular prostheses
In this expert review, Won-Keun Kim discusses key considerations for patient‑tailored transcatheter heart valve selection in index TAVI procedures, highlighting how valve type and design influence procedural success, long‑term outcomes, and lifetime management.

Patient-tailored valve selection in index TAVI
The optimal valve choice for the index transcatheter aortic valve (TAVI) procedure is crucial for immediate procedural success and safety as well as long-term outcomes and patient lifetime management - “the first cut is the deepest”. It is well known that contemporary transcatheter heart valves (THV) have different characteristics that may affect access route, deliverability, deployment, and valve function. Hence, given the anatomical variability and individual comorbidities of patients, currently, there is not one valve that fits all.
The overview in Figure 1 summarises patient-tailored selection criteria that should be considered for differential valve choice and discriminates the valve type (balloon-expandable, BE vs. self-expanding, SE) and the valve design (intra-annular vs. supra-annular).
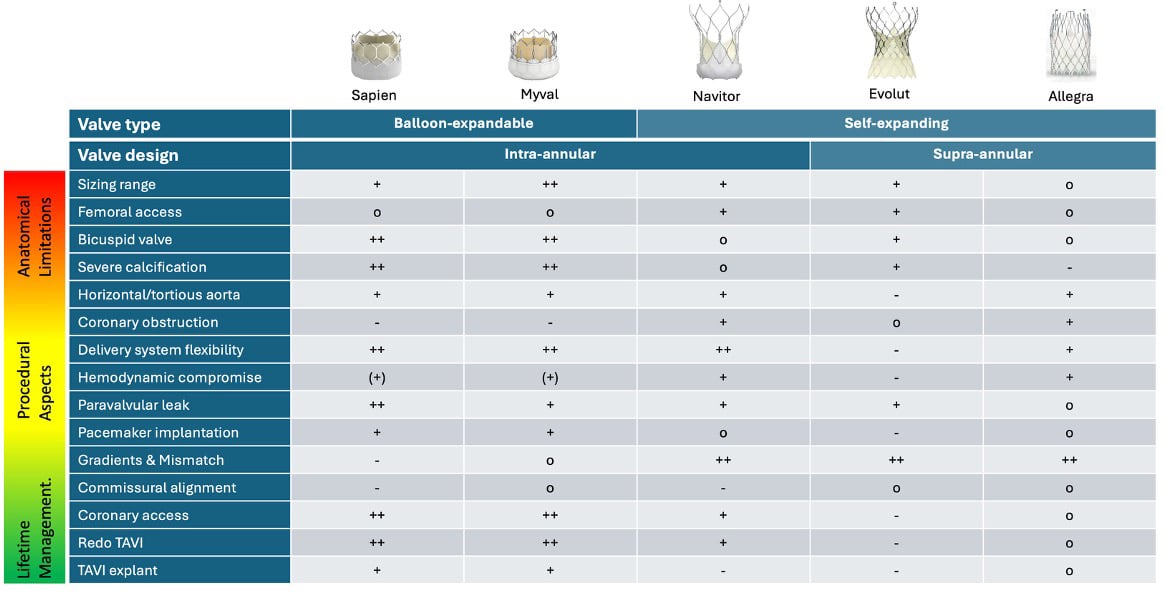
Figure 1: Criteria for customized valve selection. The matrix discriminates between balloon-expandable vs. self-expanding and intra-annular vs. supra-annular valve types. Selection criteria incorporate anatomical and procedural considerations as well as life-time management aspects.
++ very good
+ good
o acceptable
- not suitable
Importantly, not all recommendations can be backed by firm evidence. Inevitable anatomical limitations include sizing range and required femoral access diameter, whereas bicuspid aortic valve, extent and distribution of device landing zone calcification, and horizontal or tortuous aorta may be subject to device characteristics (delivery system flexibility & angulation), but also operator preference and individual experience (1,2).
Procedural and hemodynamic implications of valve type
Hemodynamic compromise during deployment is twofold: while BE devices require rapid ventricular pacing, the deployment of SE devices theoretically can be done without any pacing. However, usually short runs of rapid ventricular pacing are short and well tolerated, whereas during the deployment of SE devices, an occlusive phase with hemodynamic compromise may occur. Commonly, the extent and duration of an occlusive phase appears to be more pronounced with EVOLUT THVs due to the supra-annular leaflet position when compared to NAVITOR THVs that resume leaflet function earlier, albeit this has not been examined systematically.
Among contemporary THVs featuring sealing mechanisms, paravalvular leakage has become less relevant, but still may occur, particularly due to sizing error, malpositioning, or in the presence of severe or excentric calcification (3). For the latter, the best choice remains controversial: BE valves may provide a better sealing due to the higher radial force, but the risk of aortic root injury may be increased.
Conversely, SE valves may have a lower risk of aortic root injury but may be subject to underexpansion and paravalvular leakage (3). Conduction disturbances and permanent pacemaker implantation remain an inherent risk of TAVI given the anatomical proximity of the conduction system. Valve type and implantation depth are known to be independent predictors of these complications (4).
Even though high positioning yields lower pacemaker rates, this may be at the price of higher embolisation risk and compromised lifetime management.
Long-term considerations: coronary access and redo-TAVI
Hemodynamic performance is linked to the position (intra- vs. supra-annular) as well as the opening patterns of the prosthetic leaflets. Even though the NAVITOR THV is classified as intra-annular valve, gradients appear comparable with those of supra-annular valves (5). This may be related to the leaflet position not being strictly located in the inflow but slightly above, and due to other design considerations including the tubular stent shape and optimised leaflet opening pattern. Even though the prognostic impact of prosthesis-patient-mismatch is under debate following TAVI, it may be advisable to avoid it if possible, which is a result of valve choice, positioning, and optimal stent-frame expansion (6). Coronary access is becoming more relevant with younger patients considered for TAVI and the high prevalence of coronary artery disease among TAVI recipients. Beyond the sequence of PCI (before or after TAVI), implantation depth, and commissural alignment, the valve choice itself has major impact on coronary access (7). However, with most contemporary THVs, only passive commissural alignment is possible and not overly reliable (8).
The number of Redo-TAVI may be expected to increase in the near future. Key requisites for a straightforward Redo-TAVI procedure include design features (intra-annular, cell size, frame height), implant position and commissural alignment of the index THV, especially if coronary protection or leaflet modification is required (9). The Redo-TAVI app may be helpful for procedural planning.
It should be emphasised that selection criteria must not be valued equally, but in a hierarchical order. Thus, procedural success and safety should always have the highest priority in the decision process. If similar immediate outcomes may be expected with two different valve types, longer-term aspects can be taken into account as secondary selection criteria. Ongoing technological advancements and novel valve iterations may enhance the differential THV selection in the future.
References
- Renker M, Kim W K. Choice of transcatheter heart valve: should we select the device according to each patient's characteristics or should it be "one valve fits all"? Ann Transl Med. 2020;8:961.
- Moscarelli M, Gallo F, Gallone G, Kim W K, Reifart J, Veulemans V, Zeus T, Toggweiler S, De Backer O, Sondergaard L, Mangieri A, De Marco F, Regazzoli D, Reimers B, Muntane-Carol G, Lauriero R E, Armario X, Mylotte D, Bhadra O D, Conradi L, Donday L A M, Nombela-Franco L, Barbanti M, Reddavid C, Brugaletta S, Nicolini E, Tzanis G, Rodes-Cabau J, Colombo A, Giannini F. Aortic angle distribution and predictors of horizontal aorta in patients undergoing transcatheter aortic valve replacement. Int J Cardiol. 2021;338:58-62.
- Biroli M, Tang G H L, Taramasso M, De Marco F, Pontone G, Biancari F, Fusini L, Muratori M, Maisano F, Gennari M. Paravalvular Regurgitation After Transcatheter Aortic Valve Replacement: Incidence, Mechanism, and Interventional Management. JACC Cardiovasc Interv. 2026;19:401-421.
- Bruno F, D'Ascenzo F, Vaira M P, Elia E, Omede P, Kodali S, Barbanti M, Rodes-Cabau J, Husser O, Sossalla S, Van Mieghem N M, Bax J, Hildick-Smith D, Munoz-Garcia A, Pollari F, Fischlein T, Budano C, Montefusco A, Gallone G, De Filippo O, Rinaldi M, la Torre M, Salizzoni S, Atzeni F, Pocar M, Conrotto F, De Ferrari G M. Predictors of pacemaker implantation after transcatheter aortic valve implantation according to kind of prosthesis and risk profile: a systematic review and contemporary meta-analysis. Eur Heart J Qual Care Clin Outcomes. 2021;7:143-153.
- Worthley S G, Giordano A, Corcione N, Nombela-Franco L, De Marco F, Walton A, Bedogni F, Mollmann H, De Backer O, Leroux L, Manoharan G, Tchetche D, Taramasso M, Li L, Kuo H C, Van Mieghem N M, Investigators V S. 30-Day and 1-Year Outcomes of Navitor Transcatheter Aortic Valve in Low- or Intermediate-Risk Patients. JACC Cardiovasc Interv. 2025;18:2517-2527.
- Herrmann H C, Daneshvar S A, Fonarow G C, Stebbins A, Vemulapalli S, Desai N D, Malenka D J, Thourani V H, Rymer J, Kosinski A S. Prosthesis-Patient Mismatch in Patients Undergoing Transcatheter Aortic Valve Replacement: From the STS/ACC TVT Registry. J Am Coll Cardiol. 2018;72:2701-2711.
- Rogers T, Greenspun B C, Weissman G, Torguson R, Craig P, Shults C, Gordon P, Ehsan A, Wilson S R, Goncalves J, Levitt R, Hahn C, Parikh P, Bilfinger T, Butzel D, Buchanan S, Hanna N, Garrett R, Buchbinder M, Asch F, Garcia-Garcia H M, Okubagzi P, Ben-Dor I, Satler L F, Waksman R. Feasibility of Coronary Access and Aortic Valve Reintervention in Low-Risk TAVR Patients. JACC Cardiovasc Interv. 2020;13:726-735.
- Tang G H L, Amat-Santos I J, De Backer O, Avvedimento M, Redondo A, Barbanti M, Costa G, Tchetche D, Eltchaninoff H, Kim W K, Zaid S, Tarantini G, Sondergaard L. Rationale, Definitions, Techniques, and Outcomes of Commissural Alignment in TAVR: From the ALIGN-TAVR Consortium. JACC Cardiovasc Interv. 2022;15:1497-1518.
- Bapat V N, Fukui M, Zaid S, Okada A, Jilaihawi H, Rogers T, Khalique O, Cavalcante J L, Landes U, Sathananthan J, Tarantini G, Tang G H L, Blackman D J, De Backer O, Mack M J, Leon M B. A Guide to Transcatheter Aortic Valve Design and Systematic Planning for a Redo-TAV (TAV-in-TAV) Procedure. JACC Cardiovasc Interv. 2024;17:1631-1651.
Conflicts of interest
Personal fees from Abbott, Anteris, Biosensors, Boston Scientific, Cardiawave, Edwards Lifesciences, Jenavalve, HID Imaging, Medtronic, Meril Life Sciences, P & F. Institutional fees from Boston Scientific.
